
Abstract
This study addresses the paradoxical tensions that arise during additive manufacturing (AM) implementation for circular economy goals in the healthcare sector. Using the lens of paradox theory, this study identifies four competing priorities that stakeholders may encounter while adopting AM. Focus group discussions among 12 industry experts from the healthcare supply chain were conducted to verify the paradoxes. Semi-structured interviews were then conducted with 10 industry experts to derive the solutions to manage these tensions from an Industry 5.0 perspective to achieve the full benefits of AM. This study expands paradox theory into the AM literature and provides a novel ‘both/and’ perspective (i.e. a pluralistic rather than a dualistic perspective) to look at emerging tensions encountered while implementing AM in the healthcare sector. This perspective will help decision-makers realise that these tensions can be managed over time to turn them into creative, rather than destructive, forces.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Environmental degradation is a rapidly growing global concern and the resulting health impacts are on policy makers and industry leaders’ radars. However, the reverse has received very little attention and the environmental footprint of the healthcare sector is almost neglected. The healthcare sector, synonymous with healing, is a significant consumer of resources and energy and a major producer of emissions and waste (WHO Regional Office for Europe, 2015), thus inadvertently harming health. Such degradation is caused by direct healthcare activities (e.g., wastes from hospitals and clinics) as well as indirect activities associated with the supply chain of healthcare-related goods and services (e.g., manufacturing of healthcare instruments) (Chung & Meltzer, 2009). For example, average hospitals produce approximately 0.5 kg of waste per bed per day (United Nations Environment Programme, 2020). Hence, there is a growing urgency to accelerate global actions by the healthcare sector to adopt Circular Economy (CE) models while providing quality care to patients (van Boerdonk et al., 2021).
The concept of CE converges the ideas of biomimicry, bioprinting, industrial ecology and industrial symbiosis. These encompass product longevity, increasing the product life cycle, maximizing material value, and minimising input material, waste, emission, and energy (Philips Healthcare, 2021). To build a sustainable healthcare ecosystem, CE thinking necessitates resource productivity which can be achieved through digitalisation, such as Industry 4.0 (I4.0) (Bag et al., 2022; Pappas et al., 2018). Additive manufacturing (AM), an I4.0 technology, is a sustainable production technique that has gained much attention to facilitate CE goals (Despeisse et al., 2017). Due to its additive nature, AM minimizes resource wastage. In addition, it reduces the need for tools, fixtures, and jigs, which helps reduce resource usage. AM helps to create customised tools and equipment, as well as tailored medical devices and implants (Soares et al., 2021) that fit into the patient’s medical conditions (Aquino et al., 2018). 3D-printed patient-specific biodegradable implants dissolve inside the human body and provide better healing characteristics as compared to metal implants (Yadav et al., 2020). Moreover, AM eases repair and remanufacture processes through its modular designs, thus extending product life. Hence, it is believed that AM enables a shift towards the CE (Gao et al., 2021; Hettiarachchi et al., 2022; Wu et al., 2022) and is able to provide better sustainability benefits than traditional manufacturing practices (Khorram Niaki et al., 2022).
AM is a promising technology with strong potential to revolutionise the healthcare sector by restoring health while minimising negative impacts on the environment (Kamble et al., 2023; Gao et al., 2021; Hettiarachchi et al., 2022; Wu et al., 2022; Yadav et al., 2020). The application of AM in the healthcare sector can be witnessed across many disciplines, such as pulmonology, ophthalmology, otolaryngology, cardiovascular, oncology, oral and maxillofacial, orthopedic, and general surgery. For example, AM has been effectively used by many hospitals, such as the Walter E. Dandy Neurosurgical Society in the USA, to make surgical models which enhanced the learning curve and reduced the learning time (Stratasys, 2022). Similarly, University of Newcastle used AM and showcased optimal resource utilisation by creating 50 eye corneas using only one healthy human cornea (3dnatives, 2019). These would not have been possible with traditional manufacturing practices.
Nevertheless, AM is still an emerging technology which is plagued by numerous limitations that demand attention (Priyadarshini et al., 2022a). For instance, while AM facilitates improvements in the quality of care with personalised implants, surgical tools, and prosthetics, it also adds players (e.g., patients, surgeons, and design engineers) to the supply chain, thus increasing supply chain complexity (Blome et al., 2014). While personalisation has its environmental benefits of reduction in waste and product life extension, it also increases supply chain lead time and complexity, thus affecting supply chain responsiveness. Hence, the application of AM in the healthcare sector to achieve CE goals gives rise to certain paradoxes, which are competing priorities that exist simultaneously and persist over time (Smith & Lewis, 2011). Unless managed properly, such paradoxes can create barriers for further sustainable development of AM tools. However, engaging paradoxes effectively can lead to innovation and ambidexterity (Raisch & Birkinshaw, 2008). Therefore, while AM can be effectively used to attain CE goals in the healthcare sector, exploring and managing the paradoxes that arise in the implementation process will enable stakeholders to simultaneously integrate the benefits of these polarities while overcoming the limitations of each. It is only after comprehension of these paradoxical tensions and the imploration of solutions to manage these paradoxes that a ‘win-win’ situation for stakeholders can be created (Daddi et al., 2019). This will eventually improve overall sustainability performance of the sector. Therefore, this study adopts a paradox perspective to examine optimal implementation of AM in the healthcare sector.
In this paper, we argue that with the growth in the popularity of AM, it is important that further enhancements in the technology is done from the perspectives of Industry 5.0 (I5.0). I5.0 prioritises social well-being at every stage of the production process, and employs technologies to ensure a prosperous future that goes beyond mere economic growth and job creation (Grabowska et al., 2022). I5.0 suggests that how a technology is used is as significant as the introduction of the technology. I5.0 perspective helps to move beyond efficiency and productivity as the only goals. It emphasises the industry’s role and contribution to society (Modgil et al., 2023). Hence, I5.0 complements I4.0 by introducing the pillars of human centricity, resilience, and sustainability (European Commission, 2021).
Therefore, the solutions to paradoxes of AM implementation from an I5.0 perspective will help to incorporate the human aspect in technological advancement. This helps to move beyond the notion of just boosting the economy by AM implementation in the healthcare sector by a) making sure that healthcare activities take place within the ecological limits of the planet, b) prioritising well-being of all stakeholders involved, and c) becoming a resilient provider of continued prosperity. By ensuring that these three aspects are incorporated in solutions to the paradoxes, AM implementation can move beyond the notion of just economic growth and helps place societal well-being at the core of growth and prosperity.
Despite that, previous studies conducted focus either on the sustainability aspect of AM (Aquino et al., 2018; Yadav et al., 2020) or the performance benefits and challenges of AM in the healthcare sector (Ramola et al., 2019; Chowdhury et al., 2023). These studies fail to identify and address the paradoxical tensions that arise while implementing AM to achieve CE goals in the healthcare sector. Additionally, without making a specific reference to the paradox theory, these studies treat the paradoxes as trade-offs or dilemmas. Hence, they adopt a defensive response to paradoxical tensions that lead to undesired consequences. Therefore, to bridge research gaps based on above discussion, this study aims to answer the following research questions (RQs):
-
RQ1: What are the paradoxical tensions that arise during AM implementation in the healthcare sector for CE goals?
-
RQ2: What are the potential solutions in view of industry experts to manage these paradoxes in the Industry 5.0 context?
To answer these questions, the authors identify the paradoxes through a thorough review of the literature, thereafter, focus group discussions (FGDs) amongst industry experts are conducted to validate the paradoxical tensions. Then, semi-structured interviews with industry experts are conducted to identify the potential solutions to manage these tensions. A major contribution of this study is in identifying paradoxical tensions while implementing AM in the healthcare sector for CE goals and proposing appropriate solutions from an I5.0 perspective to manage these tensions.
It is worth noting that this study encompasses the application of AM across all disciplines of healthcare for various purposes such as pre-operative medical models, medical appliances, instruments, and parts for devices, medical tools, aids, supportive guides, splints, scaffolds, tissues, medical implants, prosthetics, and orthotics. The authors have not limited the scope to a particular medical discipline or medical application because the paradoxes that have been identified are faced across all disciplines and applications alike.
The rest of the paper is structured as follows. In the next section, the literature review has been elaborated, after which the research method is discussed. Then, the authors discuss the findings of the study and provide implications for research, practice, and policy. The paper closes with conclusions and future research directions.
2 Literature Review
The study aims to analyse the competing priorities that arise during AM implementation in the healthcare sector through the paradox theory lens and provide solutions to manage these tensions based on I5.0 core values.
2.1 Transition from Industry 4.0 Towards Industry 5.0
As the world faces an alarmingly urgent need to change its existing practices with climate change advancing at an increasing rate, industries realise the need to be environmentally sustainable (Khan & Abonyi, 2022). Moreover, global events such as the Covid-19 pandemic and the Russia-Ukraine war have brought to the forefront, the lack of preparedness in existing supply chains, thus calling for smarter and more resilient systems (Priyadarshini et al., 2022a, b). Hence, industries must review their traditional approach and design efficient and sustainable supply chains that can withstand and recover from unforeseen future disruptions. At the same time, with more technological advancements, high-value tasks that cannot be automated (e.g., creative thinking, fixing mistakes and abnormalities) will require employees to work collaboratively with technologies to make timely, efficient, and accurate decisions. This will enable humans to cultivate their unique qualities of creativity, innovation, and critical thinking, thus placing societal well-being at the core of growth and prosperity (Grabowska et al., 2022; Ericsson, 2023).
I4.0 brought in the use of technologies such as AM, artificial intelligence (AI), big data and many others focusing on advancements of automation and efficiency. However, I4.0 has a techno-economic vision focussing mainly on the role played by technologies in enhancing the efficiency of organisations, with less attention to human aspects and society (Nayeri et al., 2023). It lacks a human-centric approach and has less focus on sustainability and responsiveness (Leng et al., 2022). These limitations led to the formulation of the concept of I5.0. Unlike its predecessor, I5.0 promises an environmentally friendly, resilient, and human-centric technology-based solutions (Sindhwani et al., 2022). The European Commission acknowledged the role of I5.0 in integrating social and environmental priorities into technology-driven solutions, thus shifting the focus to a systematic approach (European Commission, 2021).
Furthermore, I5.0 also emphasizes the integration between human intelligence and machine intelligence collaboratively so that technology does not “work for us”, but rather “works with us” (Jafari et al., 2022). It aims at creating a more harmonious relationship between human and machine where technology will augment human decision-making rather than replace human employees (Karmaker et al., 2023). In this vein, researchers have now started integrating human factors while trying to facilitate technology adoption. For instance, Dora et al. (2022) used the Technology–Organisation–Environment–Human (TOEH) framework to identify and classify critical success factors for AI adoption. Similarly, Kumar et al. (2021) studied how the cognitive engagement of patients helps in obtaining adequate and customized disease management plans for patients. Sindhwani et al. (2022) suggest that the implementation of I5.0 can foster the growth of the bioeconomy, hence stimulating advancements in fields such as healthcare, medicine, surgery, genetics, and biosciences.
The adoption of I5.0 is believed to be able to lead to a future where resources are optimally utilised, firms are better equipped to tackle disruptions, and there is wider synergy between humans and autonomous machines. This can be achieved through human-centric enabling technologies and human-machine collaborations (Gladysz et al., 2023). While I4.0 is mostly technology-driven, I5.0 recognises the need for these technologies to help achieve societal values beyond jobs and growth. This can be achieved in three ways. First, by helping industries become resilient so that they can swiftly navigate through geopolitical shifts and natural emergencies (Xu et al., 2021). Second, by making production respect planetary boundaries (European Commission, 2021). Third, by placing well-being of industry workers at the centre of the production process. Hence, a more precise term for I5.0 can be society 5.0 (Grabowska et al., 2022) since it highlights the need for industries to revisit and alter their current profit-centred perspectives and strive for new strategies to cope with the changing perspectives and global climate.
Therefore, I5.0 focuses on the core values of human-centricity, sustainability and resilience, thus complementing, rather than replacing I4.0, which is largely technology-driven (Battini et al., 2022; Xu et al., 2021). Hence, the transition from I4.0 to I5.0 is multifaceted evolution that combines the technologies of I4.0 to focus on the overall well-being of the society, sustainable growth, and resilient systems.
2.2 Additive Manufacturing and I5.0
It is foreseeable, I4.0 technologies such as AM will help continue the trend of personalisation but with a greater focus on flexibility and responsiveness (Xu et al., 2021). AM, being a sustainable technology, has the potential to facilitate CE goals in the healthcare sector. First, the design freedom offered by AM enables on-demand production, thus eliminating the need for warehousing and preventing wastage due to unsold inventory. Being additive in nature, AM reduces the raw material need and wastage (Hettiarachchi et al., 2022). AM also ensures sustainability by using biomaterials and creating biodegradable implants (Yadav et al., 2020).
Second, AM has the potential to improve resilience by enabling decentralised manufacturing which saves transportation need and time, thus reducing lead time and enhancing responsiveness (Wu et al., 2022). Since modifications in the product design can be achieved by making changes to the digital design, AM enables rapid market responsiveness. AM also helps create surgical tools and guides customised to specific needs of the patients, which helps ensure medical precision, thus reducing the surgical intervention duration.
Thirdly, AM has the ability for customised medical products, which helps reduce the time required for a surgery, takes substantial burden off the medical staff, and improves the quality of life of the patients by helping them heal more quickly (Priyadarshini et al., 2023).
However, AM is still at a nascent stage with numerous technological and implementation constraints (Priyadarshini et al., 2022b). These constraints give rise to paradoxes which prevent AM from achieving its full potential. This study identifies the main paradoxes faced during the implementation of AM and provides potential solutions from an I5.0 perspective. Hence, while the paradoxes arise due to a technology-driven approach (focus of I4.0), the solutions can be obtained keeping in mind the I5.0 core values of sustainability, resilience, and human-centricity. This helps in thinking beyond solely efficiency and productivity and reinforcing the contribution of the industry to society.
2.3 Paradox Theory
In this study, we adopt paradox theory (Poole & Van de Ven, 1989) to guide our exploration. Paradoxes are tensions/inner strivings that arise due to interrelated yet conflicting demands that exist simultaneously and persist over time. In isolation, these priorities appear logical. However, when juxtaposed, they seem inconsistent, irrational, and absurd (Smith & Lewis, 2011). Emerson and Lewis (2019) observed that the human mind has been conditioned to think binary. Paradox theory enables a shift from the traditional ‘either/or’ (dualistic) thinking to a novel ‘both/and’ (pluralistic) approach (Smith & Lewis, 2011). Understanding how to navigate the space between polarities helps policy makers and industry decision-makers realise that these tensions can be managed, and, over time, can be turned into a creative force rather than a destructive one. Paradoxical tensions set off reactions that catalyse new strategic paths, which can reconfigure the supply chain while addressing the interests of conflicting stakeholders (Lewis, 2000). By doing so, the theory helps organisations to explore ways to simultaneously comply with competing priorities. In this regard, paradoxes differ from dilemmas where a choice must be made (Poole & Van de Ven, 1989).
Paradox theory has been applied to operations management research in the past. For example, Dieste et al. (2022) drew on paradox theory to identify the organisational tensions emerging during the I4.0 implementation. Carter et al. (2020) focussed on the unintended consequences of a sustainable supply chain using the paradox approach. Raisch and Krakowski (2021) explored the automation-augmentation paradox arising during artificial intelligence (AI) implementation. Erthal et al. (2021) studied the cultural tensions that arise in a healthcare organisation implementing lean. These studies have discussed the importance of using the paradox perspective to develop more nuanced interpretations and have emphasized the importance of pluralistic thinking over dualistic thinking.
Considering the stringent demands for sterility, precision, and material quality in the healthcare industry (Kamble et al., 2023), AM is a valuable tool in the effort for sustainability (Yadav et al., 2020). Nonetheless, since AM is still an evolving technology, paradoxes occur when trying to employ it to accomplish CE goals. So far, the focus of existing literature has been on the benefits, drivers, barriers, implications, and application of AM technologies. Previous literature has largely overlooked the sustainability-related paradoxes arising during AM implementation in the healthcare sector.
Therefore, this study applies paradox theory as a lens to provide deeper insights into the healthcare sector, where there is a need to adopt the paradoxical sense-making approach to provide quick and quality service while being environmentally sustainable. Frames and processes that recognise and juxtapose contradictory demands, collectively referred to as paradoxical cognition, bring underlying tensions to prominence (Smith & Tushman, 2005). Using paradox theory, researchers were able to distinguish a paradox from a trade-off which helped them to explore how to actively manage conflicting goals simultaneously (Carmine & Marchi, 2022). Engaging these tensions constructively and exploring paradoxical actions to manage them, will help in counterbalancing the defensive behaviour and lead to creativity and ambidexterity (Brix-Asala et al., 2021). In the healthcare sector, this will help in attaining the CE goals by improving the performance of AM.
Moreover, previous studies fail to discuss how these paradoxes simultaneously impact various stakeholders across the healthcare sector (e.g., Chaudhuri et al, 2023; Chowdhury et al., 2023; Khorram Niaki et al., 2022). Hence, exploring these paradoxes helps move beyond simplified notions and helps recognise the complexity and ambiguity that exists in the process of achieving CE goals through AM implementation. By adopting a rigorous, multistage process, we intend to extend the paradox theory and gain more evidence on the feasibility of a paradoxical approach in the domain of healthcare.
2.4 Identification of Paradoxical Tensions Through Literature
We first attempt to determine the paradoxes arising during AM implementation from the literature. For this purpose, we used the Scopus database due to its comprehensive collection (Norris & Oppenheim, 2007). Then, through snowballing, numerous other papers were identified and included in the study. Figure 1 shows the search syntax. The source type was limited to ‘journals’ and ‘conference proceedings.’ The subject areas were restricted to ‘Medicine,’ ‘Business and Management,’ ‘Social science’ and ‘Decision science.’ This helped in getting papers across all the key domains of the study.

Flow diagram for articles selection criteria
Figure 1 also depicts the inclusion and exclusion method for the study. The authors read the title and abstract of the 772 articles obtained from Scopus. Based on the title and abstract, only those studies that discussed the benefits, barriers, or trade-offs in AM were selected. Since the aim was to identify environmental sustainability paradoxes, the studies about the sustainability context were retained. The remaining 183 articles were then read to check their relevance to the topic under study, and accordingly, 111 articles were excluded. Then through snowballing, where reading the 72 articles lead to the identification of more relevant papers, another 49 relevant articles were added. In the end, 121 articles were used for this study.
A thorough analysis was then performed to identify paradoxical tensions in the context of CE. The consensus method was used to reach inter-rater reliability (IRR) between two or more researchers (Fink, 2010). A 7-point rating scale was used, and so long as the ratings did not differ by more than one point above or below the other researchers, the researchers were said to have reached a consensus (Stemler, 2004). Using the percentage method, the IRR was calculated to be 82% which is acceptable (McHugh, 2012). These identified tensions are shown in Table 1.
It can be seen from the table that these paradoxes are not just problems. Instead they are the ones that seems contradictory but exists simultaneously and creates tension (Smith & Lewis, 2011). These paradoxes are conflicting requirements that need to be managed simultaneously to gain the complete benefits of AM in line with the core values of I5.0 — sustainability, resilience, and human-centricity. Without creating solutions for these paradoxes, AM can still be beneficial for the healthcare sector. For example, either modularity or consolidation can not only enhance sustainability but also enhance responsiveness, despite being seemingly opposing forces. However, the paradox theory encourages paradoxical thinking to manage these tensions which entails a both/and approach rather than an either/or approach (Dieste et al., 2022). Many real-world situations require managing competing requirements and opposing forces. In this context, the paradox theory helps in understanding how to navigate and thrive in such complex environment while managing multiple contradictory demands. It helps to find ways to simultaneously pursue seemingly conflicting goals or strategies by using the best option on a case-to-case basis. This further enhances the potential of AM in achieving CE goals.
3 Research Methodology
Previous researchers have argued that a subjective approach should be taken to explore the ‘lived experiences’ and perspectives of supply chain stakeholders, especially in the case of complex processes (Turner et al., 2018). Little is known about the complex paradoxical tensions arising during AM implementation in the healthcare sector. The objective of this study is to delve into the minds and experiences of these supply chain stakeholders who must carry out an interpretation process (Daft & Weick, 1984) to identify the relevance of the paradoxes, and their impact, and ultimately suggest potential solutions from a pluralistic perspective to create win-win situations. Hence, this study utilises an interpretivist research paradigm to understand how meanings are produced, and how reality is created and enacted from the individual’s frame of reference. The authors have chosen an exploratory sequential qualitative research design (Morse, 2010; Simons et al., 2008) to delve deep into the field to investigate a novel phenomenon and enhance the theoretical understanding of the subject (Lee, 1999). Figure 2 depicts the research method used in the study.

Research method (Adapted from Loonam, 2014)
This study adopts a two-phase approach that consists of FGDs followed by semi-structured interviews with industry experts. In phase 1, FGDs were used to verify the paradoxes identified in the literature (also shown in Table 1). Identification and understanding of paradoxical tensions being a novel and complex idea, focus groups perfectly serve the purpose of this research. The popularity of focus groups can be seen in the numerous exploratory studies that have adopted the method (Dekkers et al., 2020; Belhadi et al., 2022).
In phase 2, semi-structured interviews were conducted. This ensured data collection from the industry experts to verify paradoxes and obtain additional information on the subject. An interview protocol was prepared beforehand (see Appendix Table 3). Using FGDs and semi-structured interviews helped researchers to gain meaningful insights into the nuances of the paradoxes and potential solutions to paradoxes.
3.1 Phase 1 – Focus Group Discussion
The FGDs aimed to discuss whether the paradoxes that were identified through the academic literature existed in practice. A combination of purposive and snowball sampling was followed, such that the industry experts had greater than 5 years of experience in three main areas: (i) additive manufacturing technologies, (ii) circular economy or environmental sustainability, and (iii) the healthcare sector. Moreover, as the paradoxes were encountered at different levels of the healthcare supply chain, it was necessary to have stakeholders across all levels of the supply chain to take part in the discussion since stakeholders have a variety of expectations (Gualandris et al., 2015). This would help to gain different perspectives on the paradoxes, which would then be discussed and debated to give insightful results.
While purposive sampling helped in locating the initial few experts who seemed relevant to the study, snowballing helped in getting relevant participants from various stages of the healthcare supply chain. It was also ensured that each stage of the healthcare supply chain had ample participants so that their views were not underrepresented. Experts from India and the UK were contacted through multiple channels, including LinkedIn and authors’ networks. In terms of the geographical location of the experts, India is a representative of developing countries, and the UK represents a developed country. This helped authors to get different perspectives on each paradox since the level of AM implementation, and the awareness and efforts towards CE goals vary between these countries. Including experts from both countries will allow the authors to gain a deeper understanding of the paradoxes from a wider context. Twenty-four experts willing to participate were identified. To verify the knowledge of these experts, personal profiles were checked plus preliminary discussions were held. Based on these, 12 experts were identified and included, which is sufficient, as suggested by previous researchers (Saunders et al., 2007). An overview of the participants’ profiles is provided in Appendix Table 4.
At the start of the FGD session, participants were briefed on the concept of paradox and how it differs from a dilemma. This was done mainly to help the stakeholders understand the importance of a ‘both/and’ approach as opposed to creating an ‘either/or’ strategy for the resolution of the paradoxes. The participants were promised anonymity to maximise trust and information gathering. The session lasted around 90 minutes. At the end of the session, 4 of the 6 paradoxes were retained for the study as most participants agreed on these. For the remaining 2, a consensus could not be reached because the paradoxes either seemed more like a dilemma or did not exist in practice. Hence, paradoxes V and VI (see Table 1) were dropped from the study. The results of the FGDs can be seen in Table 2 (Column 2).
3.2 Phase 2 – Semi-Structured Interview
In phase 2, the same group of experts was contacted for semi-structured interviews. Since the participants were selected after careful consideration and thorough evaluation, it seemed a logical way forward. They are considered key informants based on their knowledge of the subject and their years of experience. Neergaard and Ulhøi (2007) suggest that a smaller number of key informants is usually sufficient in achieving theoretical saturation. Krueger and Casey (2009, p. 21) refer to such people as being ‘information rich’. Previous researchers (Glaser & Strauss, 1967; Francis et al., 2010) highlighted that for interview-based studies, the appropriate sample size is a function of data saturation. Concurrent coding procedure was followed where researchers moved back and forth between interviewing and data interpretation. In this study, data saturation was reached after 8 interviews, after which the researchers conducted 2 more interviews. Hence, total of 10 experts participated in the semi-structured interviews.
Moreover, during the FGDs phase, these experts were only required to express their opinion on the existence or non-existence of a paradox with relevant arguments to back up their claim. The resolution strategies of these paradoxes were not part of the discussion of the focus group. Hence, the authors decided to approach the same set of experts who were asked about potential solutions of these paradoxes in phase 2. The interviews lasted between 35 to 120 minutes. These interviews were audio recorded after seeking consent from the participants.
A concurrent coding procedure was followed, such that the researchers moved back and forth between interviewing and data interpretation. The probing questions were modified with emerging concepts while being mindful of the research aims. Data collection was done between June 2022 and August 2022. Each interview recording was transcribed, and manual coding was done to generate thematic codes (Basit, 2003). The authors followed a methodical manual procedure of selecting significant themes that satisfy the goals and aims of the research (Papalexi et al., 2020). The initial coding was done after discussions between the two authors. The result of the initial coding was shared with the other authors, who independently checked the themes and suggested changes. After that, the authors discussed all the codes where discrepancies occurred, and a decision was taken based on the opinion of the majority.
3.3 Reliability and Validity
This study used a predetermined set of questions during the interview to ensure reliability. In this study we used data triangulation, methodological triangulation and investigator triangulation to ensure validity (Golafshani, 2003). First, we used focus group discussions and then multiple semi-structured interviews to build confidence in the findings and minimise potential bias. Second, although external validity is difficult to establish in qualitative studies (Mishra et al., 2022), this study involved representatives across various stages of the healthcare supply chain, which ensures a balanced view from multiple stakeholders and enhance the external validity of the study. These stakeholders belonged to different firms or hospitals and were from different countries, either India or the UK to ensure generalisability. Third, multiple researchers and investigators were involved in independently collecting and analysing data to ensure investigator triangulation. A rigorous process of semi-structured interviews was conducted with two researchers taking notes and transcribing interviews and other researchers checking transcripts against the recordings. In addition, using the literature as a guide and carefully drafting interview questions helped preserve content validity. Pattern matching and constructing explanations from the existing literature were used to establish internal validity.
4 Results and Discussion
This section presents the results of the data collected through interviews with industry experts. A three-stage coding process was followed. In the first stage, concepts emerged from the transcripts through open coding. Then, axial coding led to the formation of categories, and then themes emerged through selective coding (Fig. 2). After an in-depth thematic analysis, the authors used cross-referencing with academic literature to verify the themes and present research propositions based on the paradoxes and their solutions. The research propositions indicate the prevailing interpretation of the data based on the dominant themes from the semi-structured interviews. Each theme corresponds to a potential solution to manage the paradox positively. Story mapping (Loonam, 2014) was used to piece together fractured data and enable conceptualisation and sense-making. It allowed a more holistic understanding of the research inquiry. Table 2 presents the summary of the findings of the interviews. The potential solutions to manage the paradoxical tensions have been presented, along with the supply chain actors involved and the intensity of impact.
4.1 Modular Designs vs. Product Consolidation (P-I)
Experts mentioned that both product consolidation and modularity have environmental benefits. The following was mentioned by Expert 3, the president of a body that promotes AM:
Part consolidation extends the product life up to 3 times and the product weight can be reduced to one-third of the actual weight. Lightweight products reduce CO2 emissions during transportation. At the same time, lightweight implants, prosthetics, and surgical tools are also preferable to doctors and patients.
Expert 7, a product design engineer, added:
Modularity does not only enable product life extension by making repair and restoration easy but also saves time and cost. In the case of anatomical models that are used for training and preoperative surgical planning, removable (modular) structures facilitate visualisation and superior understanding of a multitude of situations.
There are healthcare products that have both interdependent designs and unique components. The experts suggested that currently, a manufacturer must take the tough selection between modularity and consolidation. Their selection mostly varies on a case-to-case basis depending upon whether there is a higher need for modularity or consolidation. Hence, they take a defensive approach that leads to undesirable consequences in the long run, such as material wastage and repeated testing and approval processes, thus wasting time. Expert 1, co-founder of an AM service-providing company, added:
This paradox ultimately leads to a compromise situation where a sacrifice in one area is made to obtain the benefits in another. For example, there are additional development costs associated with modular designs. Hence, where cost is a driving factor, modularity is not considered. Similarly, where time is a driving factor, consolidation is not considered, because approval for modular designs has already been taken.
Hence, this prevents additive manufacturing from achieving its CE goals as environmental sustainability is not always the driving factor, rather sustainability is sacrificed at times to achieve the time and cost targets. However, both modularity and consolidation of healthcare products are two sides of the same coin. Both have performance and environmental benefits, making it imperative to manage these polarities simultaneously, instead of picking one over the other (Yang & Zhao, 2018). It was also agreed upon by a majority of experts that the intensity of the impact of this paradox will be higher for larger players due to the scale of their operations and the variety of cases that they receive. When asked how this paradox can be managed, experts mentioned that design rethinking needs to be considered. Expert 2, the director of an equipment manufacturing firm, suggested:
Both product consolidation and modularity have environmental and performance benefits. To create a win-win situation, why can’t we opt for design rethinking? Create modular designs for parts where the chances of failure are high while consolidating the rest of the product.
Expert 6, the operations manager at an AM service-providing firm, added:
Testing and approval are cumbersome tasks in the medical field. Modular designs enable using the already approved and tested component in multiple products. This saves time, and cost and is environmentally favourable. At the same time, surgeons who carry out long medical procedures, prefer lightweight devices. Also, patients prefer lightweight and customisable implants. This is made possible through AM’s ability to eliminate the need for assemblies.
The expert mentioned that design rethinking creates a win-win situation in terms of performance as well as CE goals. This is based on combining function modelling with optimisation algorithms. It involves creating modular designs for parts where the chances of failure are high while consolidating the rest of the product, hence the benefits of both can be gained while overcoming their respective limitations. Kim and Moon (2020), for example, adopted this method of evaluating the feasibility of consolidation in coffee maker. Similarly, Borgue et al. (2019) tried to find the optimal trade-off between integral and modular designs. They proposed a methodology that was based on function modelling and optimisation algorithms.
Optimal resource utilisation and waste prevention are the core values of I5.0. Design rethinking enables manufacturers to incorporate sustainability principles such as design for AM (DfAM), design for sustainability and design for functionality right at the design stage. The significance of the early design stage is associated with the tasks of defining the product’s layout and its functional and operating structure (Valjak et al., 2022). Decisions made during this stage will affect the ease with which the product can be remanufactured, repaired or disassembled for recycling (De los Rios & Charnley, 2019). Hence, DfAM and design for sustainability can help manufacturers evaluate what will happen to the product at the end of its usable life.
In the healthcare sector, designing for functionality includes the serviceability time of the product. This can be done by increasing the aesthetic value via shape personalization. Designs that do not take into account the social and cultural desires of the community (such as aesthetic expectations) can result in the rejection of the prosthesis (Abbady et al., 2022). Hence, by improving the aesthetic appeal, design rethinking provides better social well-being and inclusiveness (Jiang et al., 2017). Design rethinking will also ensure a human-centric solution by saving resource and effort wastage through the production of approved and tested modular parts that fit into multiple products (Salmi, 2021), thus taking the burden of repetitive tasks off the medical staff (Kreis et al., 2022).
Design rethinking helps AM implementers combine the benefits of modularity and consolidation into the product. While modular designs for parts can save approval and testing times, consolidation can reduce the weight of the surgical instruments and tools, thus aiding in surgical intervention and reducing the operating time (Javaid & Haleem, 2020). This also saves time in critical situations, thus enhancing responsiveness which is very important for the healthcare sector (Ponomarov & Holocomb, 2009). Hence, we present the following propositions:
-
Proposition 1a.The modularity-consolidation paradox can negatively affect the benefit of AM adoption in achieving circular economy goals in the healthcare sector.
-
Proposition 1b. Design rethinking in line with I5.0 core values can reduce the negative influence of the modularity-consolidation paradox on the relationship between AM adoption and the achievement of circular economy goals in the healthcare sector.
4.2 Closing the Loop with Recycling vs. Creating High-Quality Recycled Raw Material (P-II)
Experts unanimously agreed that the science of recycled input materials is still evolving. They mentioned that the healthcare industry also needs to conform to the regulatory requirements of public health protection and infection control, thus cautioning them while using recycled materials. Expert 3, the president of a body that promotes AM, added:
Virgin materials are not only easily available but also cheap as compared to recycled materials. Sorting and recycling are costly affairs. At the same time, sterility is of utmost importance in the medical field. We want to save the environment but also protect the health of the people. Most importantly, we need to do both at low costs to be profitable.
It was mentioned that very few players are currently using recycled materials as input for AM, owing to the high costs involved and safety concerns. Experts also mentioned that the scarcity of recycled material is due to the inability of material suppliers to provide high-quality raw materials. This might be due to the lack of required technology or due to the fact that to carve a niche for themselves, some raw material suppliers deliberately limit the availability of raw materials for AM by producing materials specific to certain AM machines (Khorram Niaki & Nonino, 2017). Expert 9, founder of an AM service-providing company, suggested:
Traditional manufacturing has undergone decades of material development. With the evolution of AM, there is a need to focus on the development of the material base suitable for processing with AM machines. Currently, the raw materials are limited and the prices are very high which makes it difficult for smaller players to use recycled materials.
Experts mentioned that there is a need to develop material agnostic machines to not only bring down the cost but also for the widespread adoption of AM. Expert 3, the president of a body that promotes AM, suggested:
There should be enhanced funding for research to achieve technological innovations in terms of material processing and the development of material-agnostic machines. Through technological innovations, we need to expand the biomaterial base. Machine learning algorithms can be used to analyse the link between AM process parameters and material performance.
Experts mentioned that AM has numerous sustainability benefits as compared to traditional manufacturing practices. However, recycling is a very important aspect of circularity. While AM has huge potential for remanufacturing, repair, and refurbishing, which extends the product life (Boer et al., 2020), its capability to use recycled raw material is still limited. This causes paradoxical tensions since the stakeholders have to make a choice amongst the various R’s of CE models (Refuse, Rethink, Reduce, Reuse, Repair, Refurbish, Remanufacture, Repurpose, Recycle, and Recover) (Bag et al., 2021). Since virgin materials are easily available, actions towards developing recycled materials for AM are still limited. Hence, steps must be taken to navigate these polarities simultaneously without emphasizing only one goal (Carmine & Marchi, 2022).
Experts suggested that currently, the demand for raw materials for AM is greater than what becomes available through recycling (Wang et al., 2021). Material suppliers need to broaden the range of their products. At the same time, there is a need to develop AM machines and technology to achieve material parsimony (whole products being built from a single material), thereby supporting the eco-design concept of mono-materiality (Unruh, 2018). Expert 1, co-founder of an AM service-providing company, mentioned:
Mono materiality is the way forward. Product and packaging design needs to be investigated. We need to make sure that we are not mixing a lot of materials into the same package. For example, a metal screw cap or paper labels on a recyclable plastic bottle. There needs to be a transition to recyclable plastic labels or even printing directly on the packaging.
To address the situation, Expert 2, the director of an equipment manufacturing firm, mentioned:
It is very important to break down the bill of materials (BOM) and analyse the feedstock. Firms should strive to increase the percentage of recyclable content in their products. Then, they can make use of features like QR codes and embedded sensors that can store data about a product’s material composition and other valuable information that can show when a product is ready to be recycled, how to carry out the process, and the materials that can be reclaimed.
Expert 5, global business development manager at a firm providing AM solutions, added:
Medical device and implant manufacturers need to adopt the concept of ‘recyclable by design.’ They can use fewer different materials, and recyclable materials as input, thus making it easy to recycle at the end of the product life. For implants, biomaterials should be used. 3D bioprinting helps transform the scaffold into the tissue of interest.
Experts mentioned bio-inspired technologies and smart materials as enablers of AM adoption. These new developments allow materials with embedded sensors and enhanced features while being recyclable at the end of the product life (Xu et al., 2021). Sindhwani et al. (2022) highlight how bionics, an enabler of I5.0, can be implemented in orthopaedics, medicine, and surgery. Bionics is the science of building systems that imitate nature rather than just copying them. With the global focus on recyclability, technological advancements need to happen, and accordingly, new standards need to be developed to ensure the quality of recycled materials, especially for the healthcare sector (Ford & Despeisse, 2016; Matsumoto et al., 2016).
The concept of I5.0 highlights the importance of research and innovation to support long-term service to humanity within planetary boundaries (Xu et al., 2021). Experts mentioned that technological innovations can help the medical industry, by bringing down the cost of recycled input material. This will enable small players to use recycled raw materials as input, resulting in the inclusion of these smaller players in the game and creating job opportunities for multiple players such as recyclers and service providers (Berjozkina & Karami, 2021). At the same time, such advancements can also help recycled materials to achieve virgin-like mechanical and thermal properties and specifications, thus preventing compromising on the quality of the product (Peeters et al., 2019) and providing better care to patients.
These technological advancements to increase the material base, create material-agnostic machines, and reimagine the feedstock will introduce new players into the raw material supply chain. This will support a decentralised supply chain structure where the raw materials can be locally sourced, thus reducing the lead time and enhancing the responsiveness of the supply chain (Wu et al., 2022). Hence, even in cases of national and global supply chain disruption, recycled raw material sourcing will not be impacted.
Based on the above discussion, we present the following propositions:
-
Proposition 2a. The recycling-availability paradox can negatively affect the benefit of AM adoption in achieving circular economy goals in the healthcare sector.
-
Proposition 2b. Technological innovations (to increase the material base, develop material agnostic machines in AM, and reimagine the feedstock to increase the percentage of recyclable materials in AM) in line with I5.0 core values can reduce the negative influence of the recycling-availability paradox on the relationship between AM adoption and the achievement of circular economy goals in the healthcare sector.
4.3 Energy Savings During Production vs. Quality Management (P-III)
AM offers significant energy savings during the production process. Also, by enabling weight reduction it makes the products lighter and thus saving energy. It is estimated that the energy savings achievable by AM are considerable, between 5% and 27% of the world’s energy consumption (Verhoef et al., 2018). On the other hand, the finish quality of AM products is still a challenge due to surface roughness (Luomaranta & Martinsuo, 2020). The post-production and finishing requirements for AM are highly energy intensive because of dependencies on product geometry and application-specific requirements such as heat treatment (Oettmeier & Hofmann, 2016). This gives rise to paradoxical tensions and the polarities need to be engaged constructively to turn these tensions into a creative force which would provide immense benefits in the long run (Raisch & Birkinshaw, 2008).
Experts highlighted that the stakeholders currently consider energy saving and product quality as a trade-off, a price that must be paid. If one wants to gain the energy savings offered by AM, one must eventually perform post-processing. Hence, they focus mostly on ways to enhance post-processing activities rather than working towards eliminating the need to perform post-processing and finishing. Particularly in the healthcare industry, medical and clinical quality requirements are quite rigorous. For critical components, it is impossible to dismiss the possibility that the voids produced by the stair-stepping effect or the porous construction could serve as a microscopic refuge for germs or the virus itself. Experts suggested that this paradox will have a higher impact on larger players that use a variety of AM machines and serve a variety of industries.
Experts also suggested the use of technology for topology optimisation. When asked about the ways to address the paradox, Expert 6, the operations manager at an AM service-providing firm, responded:
Topology optimisation can be done using technologies like AI (Artificial Intelligence), which would predict distortions during the production process. This would also optimise powder flow and decreases the amount of waste powder.
Previous researchers have recommended the integration of technologies for better output. For example, Hennemann Hilario da Silva and Sehnem (2022) recommend the use of Internet of Things (IoT) for real-time energy data collection and the service of Big Data Analytics (BDA) to handle increases in generated data on intensive energy use by manufacturing industries. Wang et al. (2018) suggested using ultrasonic vibration to optimize powder delivery and decrease the wastage of powder. Thus, technology integration can lead to energy saving and better resource utilisation (Ford & Despeisse, 2016).
These technologies working in tandem will drive performance in the healthcare sector by enabling collaborative work and free up staff time to focus on higher-value tasks (Xu et al., 2021). This will prompt employees to upskill and reskill for creative problem-solving and decision-making in a dynamic environment (Nayal et al., 2022). For example, service providers should be skilled to understand the specific requirements of the surgeons. At the same time, doctors should be able to understand the design limitations of the surgical models and instruments. Hence, they can collaboratively work for value co-creation and deliver the best possible solution to the patient (Javaid & Haleem, 2020; Chaudhuri et al., 2023).
Technology integration, to overcome the respective limitation of each and combine their benefits will provide a connected system that is better equipped to handle uncertainties and thus ensures a resilient system (Qader et al., 2022). With technology integration, the sector will be better equipped to handle volatility, by combining the benefits of each technology while overcoming their respective limitations (Spieske & Birkel, 2021). With topology optimisation using AI, there can be immense time savings due to the elimination of post-processing and finishing activities. Hence, these technologies will help AM to achieve its I5.0 core values of human-centricity, sustainability and resilience rather than just being a by-product of GDP-driven prosperity development (Xu et al., 2021).
This leads us to the following proposition:
-
Proposition 3a: The energy-quality paradox can negatively affect the benefit of AM adoption in achieving circular economy goals in the healthcare sector.
-
Proposition 3b: Application of I4.0 technologies for topology optimisation in AM in line with I5.0 core values can reduce the negative influence of the energy-quality paradox on the relationship between AM adoption and the achievement of circular economy goals in the healthcare sector.
4.4 Product Personalisation vs. Responsiveness (P-IV)
The personalisation benefits of AM were extensively discussed during the interviews. The experts opined that due to personalisation, wastage is reduced. It was also mentioned that personalisation helps patients recover faster and better. Expert 5, global business development manager at a firm providing AM solutions, suggested:
In the case of implants, because the 3D-printed bones are customised, they exactly fit the curves of the human body. This not only extends the product life due to stress reduction but also enhances the recovery of the patient and reduces the chances of rejection of the implants.
Expert 4, co-founder of an AM service-providing company, added:
There is a need to save as much time as possible throughout the supply chain. Saving time will also bring down costs and make personalised products even more attractive.
However, experts also highlighted that personalisation does take time as opposed to off-the-shelf products. This is mainly because personalisation increases the supply chain complexity which in turn reduces the supply chain flexibility (Blome et al., 2014). Therefore, in time-critical situations, a choice must be made between customisation and responsiveness, even though a customised product characterises the uniqueness of the patient, reduces trials and test-fittings, quickens the healing process, and reduces the immunological rejection of implants, ultimately reducing waste. It was also suggested that this paradox will have a higher impact on smaller players due to the limited resources in collaborating with various stakeholders to improve responsiveness. Hence, there is a need to navigate these polarities constructively to gain the benefits of both.
Previous researchers suggest that mass personalisation, achieved through AM, is a criterion for assessing the enablers of I5.0. This can be achieved when the human touch is restored to manufacturing, thus achieving collaboration and human centricity (Cillo et al., 2022). I5.0 also suggests collaboration with stakeholders as a means to achieve agility and supply chain responsiveness (Nayeri et al., 2023).
Few possible solutions are mentioned in the literature and echoed by the experts. First, adopting innovative collaborative tools such as a multi-tasking facility where both the manufacturer and remanufacturer utilise the same AM equipment in the same location in close vicinity to the customer (Kunovjanek et al., 2020) can improve the flexibility and responsiveness of the system. Second, setting up point-of-care labs (POCs) at the hospital premises can reduce the time required considerably. It helps surgeons and design engineers to better collaborate to provide the best clinical outcomes (Ramola et al., 2019).
Expert 10, a surgeon who has used the technology, mentioned about the use of point-of-care labs (POCs) as an effective tool for collaboration:
Point-of-care labs (POCs) should be set up in hospitals to ensure smooth operations during personalisation. These labs can employ engineers proficient in designing products and using AM machines. Proximity to the surgeons will reduce the chances of failure while quickly providing personalised tools, devices, models, and implants to the surgeons.
This not only enhances the healthcare supply chain responsiveness but also minimizes the rejections, and hence the wastage (Wu et al., 2022). Experts suggested that POCs creates a win-win situation for all, where the patients receive personalised care, and the lead time is also reduced.
This leads to the following propositions:
-
Proposition 4a: The personalisation-responsiveness paradox can negatively affect the benefit of AM adoption in achieving circular economy goals in the healthcare sector.
-
Proposition 4b: In line with I5.0 core values, innovative collaborative tools such as POCs can reduce the negative influence of the personalisation-responsiveness paradox on the relationship between AM adoption and the achievement of circular economy goals in the healthcare sector.
However, experts also mentioned that setting up collaborative tools, such as POCs, is a challenge. First, the surgeon needs to be convinced. For example, in India, with a low doctor-to-patient ratio, surgeons are extremely busy. It was also brought to light that due to the high costs involved and lack of awareness of its benefits, hospital administration is also hesitant to set up these POCs. Expert 1, co-founder of an AM service-providing company, mentioned:
Personalisation takes time. If a hospital proposes a personalised implant to a patient and asks for 10 days, while on the other hand another hospital which has not adopted the technology, proposes to do the surgery immediately with an off-the-shelf implant, the patient is most likely to go for the second option. Moreover, the cost of personalised implants will also be high. In India, unlike Europe or USA, very few people have health insurance to cover the cost of such personalised implants.
Second, the healthcare sector typically falls under multiple compliances and regulations, such as the Food and Drug Administration (FDA) and Health Insurance Portability and Accountability Act (HIPAA) regulations of India. Such regulations may apply to the use of AM in medications and medical devices. Moreover, considering AM printers to fall under IT Systems, the Federal Government Information Security Act (FISMA) and supporting policies, such as the National Institute of Standards and Technology’s Risk Management Framework (NIST RMF), Authorization to Operate (ATO) certification and NIST Cybersecurity Framework (NIST CSF) may also apply. For example, Expert 8, co-founder of an AM service-providing company, mentioned:
When AM is used at the point of care (POC) in a hospital and anything goes wrong, there should be policies in place to fix the liability because this involves several stakeholders — machine supplier, raw material supplier and procurement team, hospital, surgeon, and the engineer in the POC who prints the implant or device.
In this sense, to ensure effective and efficient collaboration (Kamal, 2020), experts highlighted fast-tracking the regulatory approval process of 3D-printed medical devices and implants is needed to achieve a resilient healthcare ecosystem, which takes burdens off the medical staff and improves the quality of care for patients (Xu et al., 2021), while simultaneously reducing the carbon footprint of the healthcare sector.
AM is not exclusively confined to one jurisdiction especially in the healthcare sector. Efforts should be taken to save the wasteful duplication of regulatory actions and resources (Treiblmaier, 2019). The government can also frame policies to bind AM users to opt for eco-friendly materials while encouraging R&D to develop novel recycling methods to support CE (Zhu et al., 2021). Expert 5, global business development manager at a firm providing AM solutions, mentioned the following in this context:
There is a need to look at the commonalities between these regulations. Since AM comprises both digital and physical components, an apex regulation incorporating both these aspects will provide a comprehensive solution.
Experts generally highlighted the significant role of government in addressing the situation by setting up regulations and policy frameworks as well as altering them wherever necessary. Hence, the government needs to follow the “Test once, satisfy many” approach (Government of India, 2022). Experts hence highlighted the necessary changes in laws and regulations to fix liability in case of failure in the healthcare sector. This leads to the following propositions:
-
Proposition 4c: Following a “Test once, satisfy many” approach to fast-track the regulatory approval can reduce the negative influence of the personalisation-responsiveness paradox on the relationship between AM adoption and the achievement of circular economy goals in the healthcare sector.
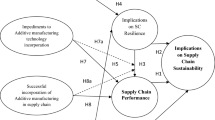
Based on the discussion and propositions, the authors present the theoretical model (Fig. 3), which depicts that AM has the potential to facilitate a circular economy in the healthcare sector. However, the paradoxes prove to be hindrances, hence they can reduce the benefits of AM adoption in achieving CE goals. Nonetheless, based on the I5.0 core values of human centricity, sustainability, and resilience, there are potential solutions to manage these paradoxes, which can reduce the negative influence of the paradoxes on the relationship between AM adoption and CE goals and facilitate I5.0 core values in the healthcare sector.

Theoretical model
5 Conclusion
This study is an early attempt to draw attention to the paradoxical tensions that arise during the application of AM in the healthcare sector to improve clinical outcomes while simultaneously striving to achieve CE goals. Based on FGDs and interviews with industry experts, the authors have verified the paradoxes and elaborated on the potential solutions in line with I5.0 core values to manage these paradoxical tensions of AM implementation. Results show that AM is still in its nascent stages, and there is a need for more research and technological innovations to make it more sustainable and affordable.
5.1 Theoretical Contributions
This study extends paradox theory to the study of AM implementation for CE goals. The study highlights the characteristics of AM, such as digital designs and manufacturing flexibility, which are beneficial to the achievement of CE goals in the healthcare sector. More importantly, this study recognizes the AM characteristics that prevent its implementations from achieving CE goals. Hence, this study identifies the competing priorities of AM implementation.
The traditional approach in dealing with these competing priorities is to take a dualistic approach where there is selection of one option or the other, even though the selection of such option varies on a case-to-case basis depending upon whether there is a higher need for one over the other. This ‘either/or’ approach prevents AM from delivering its full potential and can lead to undesirable consequences in the long run.
To address this limitation, this study explored AM implementation through the lens of paradox theory, which highlights the need for taking a ‘both/and’ (pluralistic) approach to manage competing polarities. Additionally, while navigating the management of these paradoxes, the theoretical model incorporates the three core values of I5.0 (human centricity, resilience, and sustainability). The result suggests that AM implementation following the I5.0 core values will ensure AM to reach its full potential to achieve the CE goals in the healthcare sector.
By doing so, the study dives into the interplay between cognition and paradox where after in-depth discussions with industry experts, who are themselves stakeholders across the healthcare supply chain, the study offers insights into the paradoxes. Hence, potential solutions provided in this study not only ensure the engagement of the competing polarities constructively but also improve the technology to achieve societal values beyond jobs and growth.
Our theoretical framework depicted in Fig. 3 shows the complex interplay between the potential solutions enabled by I5.0 core values of human-centricity, sustainability and resilience and the paradoxes during the AM implementation. Therefore, this paper provides further elaboration of the complex relationship between paradoxes and their solutions, which is largely missing in the current literature. This framework suggests that achieving CE goals through AM implementation in healthcare supply chains is going to be a major challenge because of the range of paradoxes and moderating factors/solutions.
5.2 Implications to Practice and Policy
The results of this study bring to the spotlight the two-way benefits of AM — lower carbon footprint and better clinical outcomes. At the same time, the study portrays how AM benefits various stakeholders across the healthcare supply chain. This study will help policy makers and senior healthcare leaders to realise the importance of incorporating I5.0 core values into AM implementation, for example, by adopting innovative collaborative tools such as POCs inside medical facilities. The results also help manufacturing companies understand how alignment between business and operational strategies will help them be economically sustainable while being environmentally friendly. Additionally, the results of the study will also help firms contemplating the adoption of AM to understand the nuances of the technology and help them make informed decisions for a smooth implementation of AM.
This study allows practitioners to grasp the benefits of the ‘both/and’ approach. The potential solutions to the paradoxes have been provided in line with I5.0 core values. With growing concerns over the power of technology outpacing human skills, this study incorporates I5.0 core values to present the human-machine symbiosis for better clinical outcomes. By doing so, the study ensures that resilience, environmental, and sociological effects of AM implementation are given the same consideration as technological advancements.
In terms of policy, this study portrays how AM, despite being developed over the years, still has related regulatory and policy frameworks in nascent stages. The results of the study draw the attention of policymakers to the need to build comprehensive policies for the smooth implementation of AM. Since the healthcare sector falls under multiple compliances and regulations, this study highlights the need for a ‘Test once, satisfy many’ approaches to prevent wasteful duplication of regulatory efforts and resources.
5.3 Limitations and Future Research
Despite the contribution to theory and practice, this study has certain limitations which deserves future research. Firstly, data collection is limited to two countries (i.e., India and UK). While these two countries are representing a developed and a developing country, including experts from more countries would widen the horizon and provide additional insights. Secondly, this study does not seek to present a cross-country comparative analysis of AM adoption; rather, it aims to converge the knowledge of all these experts to gain a comprehensive multi-stakeholder perspective. However, due to technology adoption in both countries is at different stages in terms of awareness and technology adoption, difference in opinions between experts from India and the UK could be observed. Moreover, the legal and regulatory framework for technology usage and CE goals also vary in these countries. Hence, an interesting future avenue could be a comparative study between a developed and a developing country. Thirdly, this study is exploratory, hence the propositions and the theoretical framework developed are heuristic in nature. Future quantitative studies assessing the proposed theoretical model (Fig. 3) based on multivariate techniques are encouraged. Future researchers could examine the moderating role of paradoxes in the relationship between AM implementation and the achievement of CE goals, as well as the second-order moderated moderation (i.e., conditional moderation) (Hayes, 2017; Qiao et al., 2022) role of solutions to those paradoxes in reducing the negative impact of the paradoxes. Fourthly, this study does not include patients as stakeholders in the respondents. This is because the patients would only be able to provide feedback on their experience post the implant. The patients as receiver of services would have limited views on the paradoxical tension across the healthcare supply chain. Patients may not have better views on AM benefits in comparison to traditional off-the shelf products than the doctors, because the first experience might be the only experience of the patient with implants or prosthetics. Most importantly, including patient into the study, involves much more sophisticated ethical clearance, which is out of the scope of the current study. Future researchers could try to examine the opinions of patients on AM implementation. Fifthly, paradox theory is a less explored topic in operations and supply chain management studies (Zhang et al., 2021). Future researchers can adopt the paradoxical lens to explore the tensions that arise in organisations while implementing other emerging technologies and provide solutions in line with I5.0 core values. By doing so, researchers could facilitate the organisations to view the existing tensions in a paradoxical sense-making way rather than the traditional trade-off approach for emerging technologies. Also, presenting solutions to the paradoxes in line with I5.0 core values will portray how technological advancements could benefit rather than threaten the workforce while respecting social and planetary boundaries. Hence, organisations will be able to understand the interconnections between these paradoxes to look for innovative solutions to address future challenges.
Data Availability
The original dataset is available on request.
References
3dnatives. (2019). 3D printed corneas to prevent corneal blindness. https://www.3dnatives.com/en/3d-printed-corneas-150220194. Accessed Sept 2022
Abbady, H. E., Klinkenberg, E., de Moel, L., Nicolai, N., van der Stelt, M., Verhulst, A. C., Maal, T. J., & Brouwers, L. (2022). 3D-printed prostheses in developing countries: A systematic review. Prosthetics and Orthotics International, 46(1), 19–30. https://doi.org/10.1097/PXR.0000000000000057
Adaloudis, M., & Bonnin Roca, J. (2021). Sustainability trade-offs in the adoption of 3D concrete printing in the construction industry. Journal of Cleaner Production, 307, 127201. https://doi.org/10.1016/j.jclepro.2021.127201
Aquino, R. P., Barile, S., Grasso, A., & Saviano, M. (2018). Envisioning smart and sustainable healthcare: 3D printing technologies for personalized medication. Futures, 103, 35–50. https://doi.org/10.1016/j.futures.2018.03.002
Bag, S., Gupta, S., & Kumar, S. (2021). Industry 4.0 adoption and 10R advance manufacturing capabilities for sustainable development. International Journal of Production Economics, 231, 107844. https://doi.org/10.1016/j.ijpe.2020.107844
Bag, S., Sahu, A. K., Kilbourn, P., Pisa, N., Dhamija, P., & Sahu, A. K. (2022). Modeling barriers of digital manufacturing in a circular economy for enhancing sustainability. International Journal of Productivity and Performance Management, 71(3), 833–869. https://doi.org/10.1108/IJPPM-12-2020-0637
Basit, T. (2003). Manual or electronic? The role of coding in qualitative data analysis. Educational research, 45(2), 143–154. https://doi.org/10.1080/0013188032000133548
Battini, D., Berti, N., Finco, S., Zennaro, I., & Das, A. (2022), Towards industry 5.0: A multi-objective job rotation model for an inclusive workforce. International Journal of Production Economics, 108619. https://doi.org/10.1016/j.ijpe.2022.108619
Belhadi, A., Kamble, S. S., Venkatesh, M., ChiappettaJabbour, C. J., & Benkhati, I. (2022). Building supply chain resilience and efficiency through additive manufacturing: An ambidextrous perspective on the dynamic capability view. International Journal of Production Economics, 249, 108516. https://doi.org/10.1016/j.ijpe.2022.108516
Berjozkina, G., & Karami, R. (2021). 3D printing in tourism: an answer to sustainability challenges? Worldwide Hospitality and Tourism Themes, 13(6), 773–788. https://doi.org/10.1108/WHATT-07-2021-0100
Blome, C., Schoenherr, T., & Eckstein, D. (2014). The impact of knowledge transfer and complexity on supply chain flexibility: A knowledge-based view. International Journal of Production Economics, 147, 307–316. https://doi.org/10.1016/J.IJPE.2013.02.028
Borgue, O., Panarotto, M., & Isaksson, O. (2019). Modular product design for additive manufacturing of satellite components: Maximising product value using genetic algorithms. Concurrent Engineering Research and Applications, 27(4), 331–346. https://doi.org/10.1177/1063293X19883421
Brix-Asala, C., Seuring, S., Sauer, P. C., Zehendner, A., & Schilling, L. (2021). Resolving the base of the pyramid inclusion paradox through supplier development. Business Strategy and the Environment, 30(7), 3208–3227. https://doi.org/10.1002/bse.2798
Carmine, S., & De Marchi, V. (2022). Reviewing paradox theory in corporate sustainability toward a systems perspective. Journal of Business Ethics, 184, 139–158. https://doi.org/10.1007/s10551-022-05112-2
Carter, C. R., Kaufmann, L., & Ketchen, D. J. (2020). Expect the unexpected: Toward a theory of the unintended consequences of sustainable supply chain management. International Journal of Operations and Production Management, 40(12), 1857–1871. https://doi.org/10.1108/IJOPM-05-2020-0326
Chaudhuri, A., Naseraldin, H., & Narayanamurthy, G. (2023). Healthcare 3D printing service innovation: Resources and capabilities for value Co-creation. Technovation, 121,
Chowdhury, M. M. H., Scerri, M., Shahriar, S., & Skellern, K. (2023). Digital transformation of supply chain: A study on additive manufacturing practice in medical device in Australia. Journal of Enterprise Information Management. https://doi.org/10.1108/JEIM-09-2022-0337
Chung, J. W., & Meltzer, D. O. (2009). Estimate of the carbon footprint of the US health care sector. JAMA, 302(18), 1970–1972. https://doi.org/10.1001/JAMA.2009.1610
Cillo, V., Gregori, G. L., Daniele, L. M., Caputo, F., & Bitbol-Saba, N. (2022). Rethinking companies’ culture through knowledge management lens during Industry 5.0 transition. Journal of Knowledge Management, 26(10), 2485–2498. https://doi.org/10.1108/JKM-09-2021-0718
Daddi, T., Ceglia, D., Bianchi, G., & de Barcellos, M. D. (2019). Paradoxical tensions and corporate sustainability: A focus on circular economy business cases. Corporate Social Responsibility and Environmental Management, 26(4), 770–780. https://doi.org/10.1002/csr.1719
Daft, R. L., & Weick, K. E. (1984). Toward a model of organizations as interpretation systems. Academy of Management Review, 9(2), 284–295.
De los Rios, I. C., & Charnley, F. (2019). Skills and capabilities for a sustainable and circular economy: The changing role of design. Journal of Cleaner Production, 160, 109–122. https://doi.org/10.1016/j.jclepro.2016.10.130
Dekkers, R., de Boer, R., Gelsomino, L. M., de Goeij, C., Steeman, M., Zhou, Q., Sinclair, S., & Souter, V. (2020). Evaluating theoretical conceptualisations for supply chain and finance integration: A Scottish focus group. International Journal of Production Economics, 220, 107451. https://doi.org/10.1016/J.IJPE.2019.07.024
den Boer, J., Lambrechts, W., & Krikke, H. (2020). Additive manufacturing in military and humanitarian missions: Advantages and challenges in the spare parts supply chain. Journal of Cleaner Production, 257, 120301. https://doi.org/10.1016/j.jclepro.2020.120301
Despeisse, M., Baumers, M., Brown, P., Charnley, F., Ford, S. J., Garmulewicz, A., Knowles, S., Minshall, T. H. W., Mortara, L., Reed-Tsochas, F. P., & Rowley, J. (2017). Unlocking value for a circular economy through 3D printing: A research agenda. Technological Forecasting and Social Change, 115. https://doi.org/10.1016/j.techfore.2016.09.021
Dieste, M., Sauer, P. C., & Orzes, G. (2022). Organizational tensions in industry implementation: A paradox theory approach. International Journal of Production Economics, 251, 108532. https://doi.org/10.1016/j.ijpe.2022.108532
Dora, M., Kumar, A., Mangla, S. K., Pant, A., & Kamal, M. M. (2022). Critical success factors influencing artificial intelligence adoption in food supply chains. International Journal of Production Research, 60(14), 4621–4640. https://doi.org/10.1080/00207543.2021.1959665
Engelseth, P., Salman, M., Mushtaq, W., Awaleh, F., Kozlowski, R., & Glavee-Geo, R. (2021). Additive manufacturing: currently a disruptive supply chain innovation? Operations and Supply Chain Management: An International Journal, 14(4), 410–422. https://doi.org/10.31387/oscm0470312
Emerson, B., & Lewis, K. (2019). Navigating polarities: Using both/and thinking to lead transformation. Paradoxical Press.
Ericsson (2023). Human-centric manufacturing: Industry 5.0 and the factory of the future. Accessed May 16 2023, available at: https://www.ericsson.com/en/about-us/new-world-of-possibilities/imagine-possible-perspectives/industry5-0-human-centric-manufacturing/
Erthal, A., Frangeskou, M., & Marques, L. (2021). Cultural tensions in lean healthcare implementation: A paradox theory lens. International Journal of Production Economics, 233, 107968. https://doi.org/10.1016/j.ijpe.2020.107968
European Commission, Directorate-General for Research and Innovation. (2021). Industry 5.0 – Human-centric, sustainable and resilient. Publications Office. https://data.europa.eu/doi/10.2777/073781
Fink, A. (2010). Survey research methods., International Encyclopedia of Education, 152–160. https://doi.org/10.1016/B978-0-08-044894-7.00296-7
Ford, S., & Despeisse, M. (2016). Additive manufacturing and sustainability: An exploratory study of the advantages and challenges. Journal of Cleaner Production, 137. https://doi.org/10.1016/j.jclepro.2016.04.150
Francis, J. J., Johnston, M., Robertson, C., Glidewell, L., Entwistle, V., Eccles, M. P., & Grimshaw, J. M. (2010). What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychology and Health, 25(10), 1229–1245.
Gao, C., Wolff, S., & Wang, S. (2021). Eco-friendly additive manufacturing of metals: Energy efficiency and life cycle analysis. Journal of Manufacturing Systems, 60, 459–472. https://doi.org/10.1016/j.jmsy.2021.06.011
Gladysz, B., Tran, T. A., Romero, D., van Erp, T., Abonyi, J., & Ruppert, T. (2023). Current development on the Operator 4.0 and transition towards the Operator 5.0: A systematic literature review in light of Industry 5.0. Journal of Manufacturing Systems, 70, 160–185.
Glaser, B. G., & Strauss, A. (1967). The discovery of grounded theory: Strategies for qualitative research. Aldine.
Golafshani, N. (2003). Understanding reliability and validity in qualitative research. The Qualitative Report, 8(4), 597–607.
Government of India. (2022). National strategy for additive manufacturing. Accessed September 25 2022, available at: https://www.meity.gov.in/writereaddata/files/AdditiveManufacturingBooklet14.02.2022.pdf
Grabowska, S., Saniuk, S., & Gajdzik, B. (2022). Industry 5.0: improving humanization and sustainability of Industry 4.0. Scientometrics, 127(6), 3117–3144. https://doi.org/10.1007/s11192-022-04370-1
Gualandris, J., Klassen, R. D., Vachon, S., & Kalchschmidt, M. (2015). Sustainable evaluation and verification in supply chains: Aligning and leveraging accountability to stakeholders. Journal of Operations Management, 38, 1–13. https://doi.org/10.1016/J.JOM.2015.06.002
Han, Y., Yang, Z., Ding, T., & Xiao, J. (2021). Environmental and economic assessment on 3D printed buildings with recycled concrete. Journal of Cleaner Production, 278, 123884. https://doi.org/10.1016/j.jclepro.2020.123884
Hayes, A. F. (2017). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Publications.
Hennemann Hilario da Silva, T., & Sehnem, S. (2022). The circular economy and Industry 4.0: Synergies and challenges. Revista de Gestao, 29(3), 300–313. https://doi.org/10.1108/REGE-07-2021-0121
Hettiarachchi, B. D., Brandenburg, M., & Seuring, S. (2022). Connecting additive manufacturing to circular economy implementation strategies: Links, contingencies and causal loops. International Journal of Production Economics, 246, 108414. https://doi.org/10.1016/j.ijpe.2022.108414
Huang, R., Riddle, M., Graziano, D., Warren, J., Das, S., Nimbalkar, S., Cresko, J., & Masanet, E. (2016). Energy and emissions saving potential of additive manufacturing: The case of lightweight aircraft components. Journal of Cleaner Production, 135, 1559–1570. https://doi.org/10.1016/j.jclepro.2015.04.109
Jafari, N., Azarian, M., & Yu, H. (2022). Moving from Industry 4.0 to Industry 5.0: What are the implications for smart logistics? Logistics, 6(2), 26. https://doi.org/10.3390/logistics6020026
Javaid, M., & Haleem, A. (2020). 3D printed tissue and organ using additive manufacturing: an overview, Clinical Epidemiology and Global Health, 8(2), 586–594. https://doi.org/10.1016/j.cegh.2019.12.008
Jiang, R., Kleer, R., & Piller, F. T. (2017). Predicting the future of additive manufacturing: A Delphi study on economic and societal implications of 3D printing for 2030. Technological Forecasting and Social Change, 117, 84–97. https://doi.org/10.1016/j.techfore.2017.01.006
Kamal, M. M. (2020). The triple-edged sword of COVID-19: Understanding the use of digital technologies and the impact of productive, disruptive, and destructive nature of the pandemic. Information Systems Management, 37(4), 310–317. https://doi.org/10.1080/10580530.2020.1820634
Kamble, S., Belhadi, A., Gupta, S., Islam, N., Verma, V. K., & Solima, L. (2023). Analyzing the barriers to building a 3-D printing enabled local medical supply chain ecosystem. IEEE Transactions on Engineering Management. https://doi.org/10.1109/TEM.2022.3226658
Karmaker, C. L., Bari, A. M., Anam, M. Z., Ahmed, T., Ali, S. M., de Jesus Pacheco, D. A., & Moktadir, M. A. (2023). Industry 5.0. International Journal of Production Economics, 258, 108806.
Khan, A. A., & Abonyi, J. (2022). Information sharing in supply chains – Interoperability in an era of circular economy. Cleaner Logistics and Supply Chain, 5, 100074. https://doi.org/10.1016/j.clscn.2022.100074
Khorram Niaki, M., & Nonino, F. (2017). Additive manufacturing management: A review and future research agenda. International Journal of Production Research, 55(5), 1419–1439. https://doi.org/10.1080/00207543.2016.1229064
Khorram Niaki, M., Nonino, F., Tafakkori, K., Torabi, S. A., & Kazemian, I. (2022). The influence of manufacturing contexts on additive manufacturing-enabled competitive capabilities. Journal of Manufacturing Technology Management, 33(6), 1102–1123. https://doi.org/10.1108/JMTM-07-2021-0241
Kim, S., & Moon, S. K. (2020). A part consolidation design method for additive manufacturing based on product disassembly complexity. Applied Sciences (Switzerland), 10(3). https://doi.org/10.3390/app10031100
Kreis, A., Walzel, B., Schäfer, U., & Hirz, M. (2022). Onsite medical implants creation by combination of enhanced design methods and 3D printing. Computer-Aided Designs and Applications, 19(2), 336–345. https://doi.org/10.14733/cadaps.2022.336-345
Krueger, R., & Casey, M. (2009). Focus groups: A Practical guide for applied research. Sage Publications.
Kumar, P., Dwivedi, Y. K., & Anand, A. (2021). Responsible artificial intelligence (AI) for value formation and market performance in healthcare: The mediating role of patient’s cognitive engagement. Information Systems Frontiers. https://doi.org/10.1007/s10796-021-10136-6
Kunovjanek, M., Knofius, N., & Reiner, G. (2020). Additive manufacturing and supply chains–A systematic review. Production Planning and Control, 1–21. https://doi.org/10.1080/09537287.2020.1857874
Lee, T. W. (1999). Using qualitative methods in organizational research. Sage Publications.
Leng, J., Sha, W., Wang, B., Zheng, P., Zhuang, C., Liu, Q., Wuest, T., Mourtzis, D., & Wang, L. (2022). Industry 5.0: Prospect and retrospect. Journal of Manufacturing Systems, 65, 279–295.
Lewis, M. W. (2000). Exploring paradox: Toward a more comprehensive guide. The Academy of Management Review, 25(4), 760. https://doi.org/10.2307/259204
Liu, W., Deng, K., Wei, H., Zhao, P., Li, J., & Zhang, Y. (2021). A decision-making model for comparing the energy demand of additive-subtractive hybrid manufacturing and conventional subtractive manufacturing based on life cycle method. Journal of Cleaner Production, 311, 127795. https://doi.org/10.1016/j.jclepro.2021.127795
Loonam, J. (2014). Towards a grounded theory methodology: Reflections for management scholars. Irish Journal of Management, 33(1), 49.
Luomaranta, T., & Martinsuo, M. (2020). Supply chain innovations for additive manufacturing. International Journal of Physical Distribution and Logistics Management, 50(1), 54–79. https://doi.org/10.1108/IJPDLM-10-2018-0337
Matsumoto, M., Yang, S., Martinsen, K., & Kainuma, Y. (2016). Trends and research challenges in remanufacturing. International Journal of Precision Engineering and Manufacturing - Green Technology, 3(1), 129–142. https://doi.org/10.1007/s40684-016-0016-4
McHugh, M. L. (2012). Interrater reliability: The Kappa statistic. Biochemia Medica, 22(3), 276. https://doi.org/10.11613/bm.2012.031
Mishra, R., Singh, R. K., & Song, M. (2022). Managing tensions in resilience development: A paradox theory perspective on the role of digital transformation. Journal of Enterprise Information Management.https://doi.org/10.1108/JEIM-08-2022-0271
Modgil, S., Singh, R. K., & Agrawal, S. (2023). Developing human capabilities for supply chains: An industry 5.0 perspective. Annals of Operations Research, pp. 1–31. https://doi.org/10.1007/s10479-023-05245-1
Morse, J. M. (2010). Simultaneous and sequential qualitative mixed method designs what is a mixed method design? Qualitative Inquiry, 16(6), 483–491. https://doi.org/10.1177/1077800410364741
Nayal, P., Pandey, N., & Paul, J. (2022). Covid-19 pandemic and consumer-employee-organization wellbeing: A dynamic capability theory approach. Journal of Consumer Affairs, 56(1), 359–390. https://doi.org/10.1111/joca.12399
Nayeri, S., Sazvar, Z., & Heydari, J. (2023). Towards a responsive supply chain based on the industry 5.0 dimensions: A novel decision-making method. Expert Systems with Applications, 213, 119267. https://doi.org/10.1016/j.eswa.2022.119267
Neergaard, H., & Ulhøi, J. P. (Eds.). (2007). Handbook of qualitative research methods in entrepreneurship. Edward Elgar Publishing.
Norris, M., & Oppenheim, C. (2007). Comparing alternatives to the web of science for coverage of the social sciences’ literature. Journal of Informetrics, 1(2), 161–169. https://doi.org/10.1016/j.joi.2006.12.001
Oettmeier, K., & Hofmann, E. (2016). Impact of additive manufacturing technology adoption on supply chain management processes and components. Journal of Manufacturing Technology Management, 27(7). https://doi.org/10.1108/JMTM-12-2015-0113
Padmanabhan, A., & Zhang, J. (2018). Cybersecurity risks and mitigation strategies in additive manufacturing. Progress in Additive Manufacturing, 3(1–2), 87–93. https://doi.org/10.1007/S40964-017-0036-9
Papalexi, M., Bamford, D., & Breen, L. (2020). Key sources of operational inefficiency in the pharmaceutical supply chain. Supply Chain Management: An International Journal, 25(6), 617–635. https://doi.org/10.1108/SCM-02-2019-0076
Pappas, I. O., Mikalef, P., Giannakos, M. N., Krogstie, J., & Lekakos, G. (2018). Big data and business analytics ecosystems: Paving the way towards digital transformation and sustainable societies. Information Systems and E-Business Management, 16(3), 479–491. https://doi.org/10.1007/s10257-018-0377-z
Peeters, B., Kiratli, N., & Semeijn, J. (2019). A barrier analysis for distributed recycling of 3D printing waste: Taking the maker movement perspective. Journal of Cleaner Production, 241, 118313. https://doi.org/10.1016/j.jclepro.2019.118313
Philips Healthcare. (2021). Why circular design is essential for better healthcare. https://www.philips.com/a-w/about/news/archive/blogs/innovation-matters/2021/20210721-why-circular-design-is-essential-for-better-healthcare.html. Accessed Sept 2022
Ponomarov, S. Y., & Holcomb, M. C. (2009). Understanding the concept of supply chain resilience. The International Journal of Logistics Management, 20(1), 124–143. https://doi.org/10.1108/09574090910954873
Poole, M. S., & Van de Ven, A. H. (1989). Using paradox to build management and organization theories. Academy of Management Review, 14(4), 562–578. https://doi.org/10.5465/amr.1989.4308389
Priyadarshini, J., Singh, R. K., Mishra, R., & Bag, S. (2022). Investigating the interaction of factors for implementing additive manufacturing to build an antifragile supply chain : TISM - MICMAC approach. Operations Management Research, 15, 567–588. https://doi.org/10.1007/s12063-022-00259-7
Priyadarshini, J., Singh, R. K., Mishra, R., & Kamal, M. M. (2022). Adoption of additive manufacturing for sustainable operations in the era of circular economy: Self-assessment framework with case illustration. Computers & Industrial Engineering, 171, 108514.
Priyadarshini, J., Singh, R. K., Mishra, R., & Dora, M. (2023). Application of additive manufacturing for a sustainable healthcare sector: Mapping current research and establishing future research agenda. Technological Forecasting and Social Change, 194, 122686.
Qader, G., Junaid, M., Abbas, Q., & Mubarik, M. S. (2022). Industry 4.0 enables supply chain resilience and supply chain performance. Technological Forecasting and Social Change, 185, 122026. https://doi.org/10.1016/j.techfore.2022.122026
Qiao, J., Li, S., & Capaldo, A. (2022). Green supply chain management, supplier environmental commitment, and the roles of supplier perceived relationship attractiveness and justice. A moderated moderation analysis. Business Strategy and the Environment, 31(7), 3523–3541.
Raisch, S., & Birkinshaw, J. (2008). Organizational ambidexterity: Antecedents, outcomes, and moderators. Journal of Management, 34(3), 375–409. https://doi.org/10.1177/0149206308316058
Raisch, S., & Krakowski, S. (2021). Artificial intelligence and management: The automation–augmentation paradox. Academy of Management Review, 46(1), 192–210. https://doi.org/10.5465/AMR.2018.0072
Ramola, M., Yadav, V., & Jain, R. (2019). On the adoption of additive manufacturing in healthcare: A literature review. Journal of Manufacturing Technology Management, 20(1), 48–69. https://doi.org/10.1108/JMTM-03-2018-0094
Rinaldi, M., Caterino, M., Fera, M., Manco, P., & Macchiaroli, R. (2021). Technology selection in green supply chains - The effects of additive and traditional manufacturing. Journal of Cleaner Production, 282, 124554. https://doi.org/10.1016/j.jclepro.2020.124554
Rogers, H., & Srivastava, M. (2021). Emerging sustainable supply chain models for 3d food printing. Sustainability (Switzerland), 13(21), 12085. https://doi.org/10.3390/su132112085
Salmi, M. (2021). Additive manufacturing processes in medical applications. Materials, 14(1), 191. https://doi.org/10.3390/ma14010191
Saunders, M., Lewis, P., & Thornhill, A. (2007). Research methods for business students Edinburgh, Pearson Education Limited.
Simons, L., Lathlean, J., & Squire, C. (2008). Shifting the focus: Sequential methods of analysis with qualitative data. Qualitative Health Research, 18(1), 120–132. https://doi.org/10.1177/1049732307310264
Sindhwani, R., Afridi, S., Kumar, A., Banaitis, A., Luthra, S., & Singh, P. L. (2022). Can industry 5.0 revolutionize the wave of resilience and social value creation? A multi-criteria framework to analyze enablers. Technology in Society, 68, 101887. https://doi.org/10.1016/j.techsoc.2022.101887
Smith, W. K., & Lewis, M. W. (2011). Toward a theory of paradox: A dynamic equilibrium model of organizing. Academy of Management Review, 36(2), 381–403. https://doi.org/10.5465/amr.2011.59330958
Smith, W. K., & Tushman, M. L. (2005). Managing strategic contradictions: A top management model for managing innovation streams. Organization science, 16(5), 522–536. https://doi.org/10.1287/orsc.1050.0134
Soares, B., Ribeiro, I., Cardeal, G., Leite, M., Carvalho, H., & Peças, P. (2021). Social life cycle performance of additive manufacturing in the healthcare industry: The orthosis and prosthesis cases industry: The orthosis and prosthesis cases. International Journal of Computer Integrated Manufacturing, 34(3), 327–340. https://doi.org/10.1080/0951192X.2021.1872100
Spieske, A., & Birkel, H. (2021). Improving supply chain resilience through industry 4.0: A systematic literature review under the impressions of the COVID-19 pandemic. Computers & Industrial Engineering, 158, 107452. https://doi.org/10.1016/j.cie.2021.107452
Stemler, S. E. (2004). A comparison of consensus, consistency, and measurement approaches to estimating interrater reliability. Practical Assessment, Research and Evaluation, 9(1), 4. https://doi.org/10.7275/96jp-xz07
Stratasys. (2022). 3D printed brain models. https://www.stratasys.com/en/stratasysdirect/resources/case-studies/3d-printed-brain-models-walter-e-dandy-neurosurgical-society/. Accessed Nov 2022
Treiblmaier, H. (2019). Combining blockchain technology and the physical internet to achieve triple bottom line sustainability: A comprehensive research agenda for modern logistics and supply chain management. Logistics, 3(1), 10. https://doi.org/10.3390/logistics3010010
Turner, N., Aitken, J., & Bozarth, C. (2018). A framework for understanding managerial responses to supply chain complexity. International Journal of Operations & Production Management, 38(6), 1433–1466.
United Nations Environment Programme. (2020). Healthcare waste: what to do with it? https://www.unep.org/news-and-stories/story/healthcare-waste-what-do-it. Accessed Sept 2022
Unruh, G. (2018). Circular economy, 3D printing, and the biosphere rules. California Management Review, 60(3), 95–111. https://doi.org/10.1177/0008125618759684
Valjak, F., Kosorčić, D., Rešetar, M., & Bojčetić, N. (2022). Function-based design principles for additive manufacturing. Applied Sciences (Switzerland), 12(7), 1–17. https://doi.org/10.3390/app12073300
van Boerdonk, P. J. M., Krikke, H. R., & Lambrechts, W. (2021). New business models in circular economy: A multiple case study into touch points creating customer values in health care. Journal of Cleaner Production, 282, 125375. https://doi.org/10.1016/j.jclepro.2020.125375
Verboeket, V., Zuyd, H., Khajavi, S., Krikke, H. R., Nederland, O. U., & Salmi, M. (2021). Additive manufacturing for localized medical parts production: A case study. IEEE Access, 9, 25818–25834. https://doi.org/10.1109/ACCESS.2021.3056058
Verhoef, L. A., Budde, B. W., Chockalingam, C., García Nodar, B., & van Wijk, A. J. M. (2018). The effect of additive manufacturing on global energy demand: An assessment using a bottom-up approach. Energy Policy, 112, 349–360. https://doi.org/10.1016/J.ENPOL.2017.10.034
Wang, W., Pinkerton, A. J., & Li, L. (2018). A gas-free powder delivery system for 100% deposition efficiency in direct laser deposition. International Congress on Applications of Lasers & Electro-Optics, 1, 801. https://doi.org/10.2351/1.5061341
Wang, Y., Ahmed, A., Azam, A., Bing, D., Shan, Z., Zhang, Z., Tariq, M. K., Sultana, J., Mushtaq, R. T., Mehboob, A., Xiaohu, C., & Rehman, M. (2021). Applications of additive manufacturing (AM) in sustainable energy generation and battle against COVID-19 pandemic: The knowledge evolution of 3D printing. Journal of Manufacturing Systems, 60, 709–733. https://doi.org/10.1016/j.jmsy.2021.07.023
WHO Regional Office for Europe. (2015). Environmentally Sustainable Health Systems. Accessed September 25 2022, available at: http://www.euro.who.int/en/health-topics/environment-and-health/Climate-change/publications/2015/environmentally-sustainable-health-systems.-meeting-report.-11-12-november-2015,-bonn,-germany
Wu, H., Mehrabi, H., Naveed, N., & Karagiannidis, P. (2022). Impact of strategic control and supply chain management on recycled plastic additive manufacturing. Journal of Cleaner Production, 364, 132511. https://doi.org/10.1016/j.jclepro.2022.132511
Xu, X., Lu, Y., Vogel-Heuser, B., & Wang, L. (2021). Industry 4.0 and Industry 5.0—Inception, conception and perception. Journal of Manufacturing Systems, 61, 530–535. https://doi.org/10.1016/j.jmsy.2021.10.006
Yadav, D., Garg, R. K., Ahlawat, A., & Chhabra, D. (2020). 3D Printable biomaterials for orthopedic implants: Solution for sustainable and circular economy. Resources Policy, 68, 101767. https://doi.org/10.1016/j.resourpol.2020.101767
Yang, S., & Zhao, Y. F. (2018). Additive manufacturing-enabled part count reduction: A lifecycle perspective. Journal of Mechanical Design, 140(3). https://doi.org/10.1115/1.4038922
Zhang, J., Yalcin, M. G., & Hales, D. N. (2021). Elements of paradoxes in supply chain management literature: A systematic literature review. International Journal of Production Economics, 232, 107928. https://doi.org/10.1016/j.ijpe.2020.107928
Zhu, C., Li, T., Mohideen, M. M., Hu, P., Gupta, R., Ramakrishna, S., & Liu, Y. (2021). Realization of circular economy of 3D printed plastics: A review. Polymers, 13(5), 1–16. https://doi.org/10.3390/polym13050744
Acknowledgements
The authors would like to thank the editorial team and the anonymous reviewers for their valuable input and constructive suggestions. The authors would also like to thank the participating experts for their knowledge and cooperation.
Author information
Authors and Affiliations
Contributions
Jaya Priyadarshini – Conceptualization, Methodology, Data collection, Analysis Writing up.
Rajesh Kr Singh – Conceptualization, Methodology, Data collection, Analysis, Writing up.
Ruchi Mishra – Conceptualization, Methodology, Analysis, Writing up.
Qile He – Conceptualization, Methodology, Analysis, Writing up.
Ashley Braganza – Conceptualization, Methodology, Writing up.
Corresponding authors
Ethics declarations
Ethics Approval and Consent to Participate
The authors have obtained ethics approval from the home institution regarding this research. Consent has been obtained from all participants to the study.
Consent for Publication
N/A.
Competing Interest
The authors have no relevant financial or non-financial interests to disclose.
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix 1
Appendix 1
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Priyadarshini, J., Singh, R.K., Mishra, R. et al. Implementation of Additive Manufacturing in the Healthcare Supply Chain for Circular Economy Goals: Paradoxical Tensions and Solutions from an Industry 5.0 Perspective. Inf Syst Front (2024). https://doi.org/10.1007/s10796-024-10482-1
Accepted:
Published:
DOI: https://doi.org/10.1007/s10796-024-10482-1