
Abstract
Aims/hypothesis
Obesity surgery (OS) and diet-induced weight loss rapidly improve insulin resistance. We aim to investigate the impact of either Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy (SG) surgery compared with a diet low in energy (low-calorie diet; LCD) on body composition, glucose control and insulin sensitivity, assessed both at the global and tissue-specific level in individuals with obesity but not diabetes.
Methods
In this parallel group randomised controlled trial, patients on a waiting list for OS were randomised (no blinding, sealed envelopes) to either undergo surgery directly or undergo an LCD before surgery. At baseline and 4 weeks after surgery (n=15, 11 RYGB and 4 SG) or 4 weeks after the start of LCD (n=9), investigations were carried out, including an OGTT and hyperinsulinaemic–euglycaemic clamps during which concomitant simultaneous whole-body [18F]fluorodeoxyglucose-positron emission tomography (PET)/MRI was performed. The primary outcome was HOMA-IR change.
Results
One month after bariatric surgery and initiation of LCD, both treatments induced similar reductions in body weight (mean ± SD: −7.7±1.4 kg and −7.4±2.2 kg, respectively), adipose tissue volume (7%) and liver fat content (2% units). HOMA-IR, a main endpoint, was significantly reduced following OS (−26.3% [95% CI −49.5, −3.0], p=0.009) and non-significantly following LCD (−20.9% [95% CI −58.2, 16.5). For both groups, there were similar reductions in triglycerides and LDL-cholesterol. Fasting plasma glucose and insulin were also significantly reduced only following OS. There was an increase in glucose AUC in response to an OGTT in the OS group (by 20%) but not in the LCD group. During hyperinsulinaemia, only the OS group showed a significantly increased PET-derived glucose uptake rate in skeletal muscle but a reduced uptake in the heart and abdominal adipose tissue. Both liver and brain glucose uptake rates were unchanged after surgery or LCD. Whole-body glucose disposal and endogenous glucose production were not significantly affected.
Conclusions/interpretation
The short-term metabolic effects seen 4 weeks after OS are not explained by loss of body fat alone. Thus OS, but not LCD, led to reductions in fasting plasma glucose and insulin resistance as well as to distinct changes in insulin-stimulated glucose fluxes to different tissues. Such effects may contribute to the prevention or reversal of type 2 diabetes following OS. Moreover, the full effects on whole-body insulin resistance and plasma glucose require a longer time than 4 weeks.
Trial registration
ClinicalTrials.gov NCT02988011
Funding
This work was supported by AstraZeneca R&D, the Swedish Diabetes Foundation, the European Union’s Horizon Europe Research project PAS GRAS, the European Commission via the Marie Sklodowska Curie Innovative Training Network TREATMENT, EXODIAB, the Family Ernfors Foundation, the P.O. Zetterling Foundation, Novo Nordisk Foundation, the Agnes and Mac Rudberg Foundation and the Uppsala University Hospital ALF grants
Graphical Abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.

Introduction
Over recent decades, the prevalence of obesity has increased dramatically, reaching pandemic levels worldwide, there being over 1.9 billion adults with overweight or obesity in 2016 [1]. Overweight and obesity are characterised by an excessive accumulation of body fat, which, together with an unfavourable distribution, significantly contributes to various health issues, including perturbed glucose and lipid metabolism in insulin-sensitive tissues, leading to type 2 diabetes and dyslipidaemia. Additionally, it increases the risk for several comorbidities, including hypertension, major cardiovascular events, renal impairment and several cancer forms, as well as hepatobiliary, musculoskeletal and psychiatric diseases [1,2,3,4]. Effective interventions are crucial to combat obesity and its associated comorbidities. Pharmaceutical options such as semaglutide and tirzepatide, which mimic gastrointestinal (GI) hormones, show promise, although their long-term efficacy and safety warrant further investigation [5]. Obesity surgery (OS) and diets low in energy (low-calorie diets; LCDs) have demonstrated substantial weight loss and reduced obesity-related morbidity and mortality [6, 7].
Several surgical options, including Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG), involve gastrointestinal tract rearrangements and reduce energy intake and uptake [8]. RYGB is particularly efficient for long-term weight loss [9, 10] and prevention or reversal of type 2 diabetes [11, 12]. OS also mitigates other obesity-related comorbidities, such as CVD, fatty liver disease and sleep apnoea [7,8,9, 13, 14], and improves quality of life [7, 13]. The cardiometabolic benefits of OS (e.g. a rapid effect on glucose homeostasis) are partly independent of weight loss [14]. Thus, OS is commonly termed metabolic surgery [12, 15], although the mechanisms for its diverse benefits remain incompletely understood [14], with some studies proposing a potential role of the brain [16, 17].
On the other hand, LCDs are commonly recommended as the primary approach for weight loss [18]. Several diet principles aim to reduce daily energy intake [19]. While nutritionally balanced and individually customised LCDs can improve glycaemic control, liver fat content, BP and lipid profiles [20], long-term adherence and weight maintenance are challenging [9, 21,22,23].
Limited evidence exists of the short-term comparative effectiveness of diet- and surgery-based interventions for weight loss and their effects on glucose and lipid handling in different tissues. Therefore, this RCT aimed to investigate the metabolic effects observed 4 weeks after OS or the initiation of LCD, with a special focus on tissue-specific glucose uptake and metabolism. We combined traditional gold-standard metabolic assessments, such as the OGTT and the hyperinsulinaemic–euglycaemic clamp, with simultaneous [18F]fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) and MRI to assess glucose turnover in individual tissues and body fat content and distribution. We hypothesised that OS would rapidly improve insulin sensitivity, as evidenced by the glucose clamp test, largely through a reduction in endogenous glucose production (EGP).
Methods
Participants
Thirty non-diabetic patients (28 women, 2 men (self-reported); BMI 35–45 kg/m2) planned to undergo an obesity surgery were recruited at the Department of Endocrinology and Diabetes, Uppsala University Hospital, Uppsala, Sweden, during a pre-surgical endocrinological assessment. Exclusion criteria included diabetes, other endocrine disorders (except well-treated hypothyroidism), cancer, previous cardiovascular events, untreated sleep apnoea, major illnesses and pregnancy. The study consisted of a parallel-group randomised controlled trial. The participants were randomly assigned to two arms: (1) OS (RYGB or SG by patient decision) without presurgical diet change; or (2) LCD for 4 weeks, followed by OS. The OS/LCD allocation ratio was initially 1:1, later altered to 2:1. The allocation sequence was obtained using sequentially numbered, sealed envelopes, which were kept by a research nurse. Neither study participants nor caregivers and study investigators were blind to the group assignment. Six participants withdrew before or during the baseline investigations, due to reasons such as back pain, claustrophobia and lack of venous access (Fig. 1). Ultimately, 15 participants in the OS arm and nine in the LCD arm completed the 4 week intervention and follow-up, albeit one could not complete clamps with PET/MRI (LCD group; due to claustrophobia). The study participants were representative of the population undergoing obesity surgery in terms of sex and age distribution. The study adhered to Consolidated Standards of Reporting Trials (CONSORT) guidelines [24]. The Regional Ethics Review Board in Uppsala approved the study (Dnr 2015/514 with amendment 2015/514/1). All participants provided written informed consent (ClinicalTrials.gov registration no. NCT02988011) and investigations followed the principles of the Declaration of Helsinki (2008).

CONSORT diagram. Flow chart showing participant progression. For details, see Methods
Experimental design
Participants were assessed at baseline and 4 weeks post LCD or surgery. In the surgery group, 15 participants were offered RYGB or SG. The LCD consisted of liquid meal (Modifast; Täby, Sweden) replacements for 4 weeks, providing 4600 kJ (1100 kcal) energy intake per day. Both groups aimed for 8–10% weight loss [22, 25]. The primary outcome was HOMA-IR change. Secondary outcomes included anthropometric measures (weight, waist and hip circumference, and body fat % measured by bioimpedance using Tanita BC-418 [Tanita Corporation, Tokyo, Japan]), blood tests, subcutaneous adipose tissue (SAT) needle biopsy, 2 h 75 g OGTT, hyperinsulinaemic–euglycaemic clamp with glucose uptake assessment with 18F-FDG-PET, and 24 h physical activity and energy expenditure. See electronic supplementary material (ESM) Methods for additional details.
Hyperinsulinaemic–euglycaemic clamp
A hyperinsulinaemic–euglycaemic clamp was performed, as previously reported to be compatible with whole-body PET/MRI [26, 27]. In brief, human insulin (Actrapid; Novo Nordisk, Copenhagen, Denmark) was infused at 56 mU (m2 body surface)−1 min−1, and plasma insulin levels were raised to about 700 pmol/l. A variable glucose infusion (200 mg/ml) was simultaneously adjusted to maintain stable plasma glucose at 5.6 mmol/l. The M value, reflecting whole-body insulin sensitivity, was derived from the glucose infusion rate during the clamp steady state (60–120 min) and calculated as glucose infusion rate per lean body mass (LBM) (mg [kg LBM]−1 min−1).
PET/MRI acquisition
We used a whole-body integrated simultaneous 3.0 T PET/MRI system (Signa PET/MR; GE Healthcare, Waukesha, WI, USA) following an established protocol [27, 28]. Initially, 4 MBq of 18F-FDG per kg of body weight was injected for a 10 min dynamic PET scan focusing on early 18F-FDG dynamics in the thorax. Subsequently, five static whole-body PET scans, covering head to toe, were conducted with ten bed positions, each lasting 30 s. Simultaneously acquired water-fat (Dixon) MRI data, using vendor-specific magnetic resonance attenuation correction (MRAC) sequence, facilitated PET data attenuation correction and whole-body tissue segmentation. MRAC generated two distinct whole-body image datasets: a water signal image; and a fat signal image. Comprehensive corrections for quantitative PET evaluation, including random and scatter corrections, were executed. After PET/MRI scans, we performed two dedicated water-fat MRI acquisitions of the liver and pancreas using a 3D six-echo gradient-echo acquisition and a vendor-specific water-fat reconstruction method (iterative decomposition of fat and water with echo asymmetry and least squares estimation [IDEAL-IQ) [29]). This sequence produced quantitative fat fraction images with voxel intensities representing the fraction of the fat signal to the total water and fat signal.
PET/MRI-derived quantifications
Quantitative 18F-FDG net glucose influx rate Ki images were generated. Whole-body glucose disposal (Rd), EGP and specific tissue glucose metabolic rate (MRglu) were calculated based on 18F-FDG kinetics, tissue lumped constants and adjustment for urinary and blood 18F-FDG, as previously reported [26, 29]. Adipose and non-adipose tissue volumes were quantified from whole-body water-fat MRI using automated image analysis. Liver and pancreatic fat % were quantified from manually delineated fat fraction maps. See ESM Methods for details.
Statistical analyses
Data are displayed as mean ± SD unless otherwise indicated. All data were first checked for normality using Shapiro–Wilk test and normal distribution of the residuals was analysed by visual validation of Q–Q plots. Homoscedasticity was deemed acceptable after visual inspection of residuals vs predicted values. Non-normally distributed data were log-transformed before analysis. Back-transformation to the original scale was made and results display geometric mean and CI (95% CI). Group differences at baseline between the surgery and LCD group and changes from baseline within a group were analysed using independent t test and paired t test, respectively. Analyses of change from baseline between the groups (surgery vs LCD) were assessed with ANCOVA adjusted for the outcome baseline value. Comparison between the number of participants with normoglycaemia or prediabetes between OS and LCD was performed with Fisher’s Exact test. For this exploratory research focusing on potential mechanisms there was no formal prespecified power requirement. However, power analyses based on previous studies [30, 31], indicate that the current sample size in the LCD group (n=9) gives 80% power to detect a change from baseline in fasting plasma glucose of 0.53 mmol/l and HOMA-IR of 2.2 units, with α=0.05. The larger OS group (n=15) provides more than 80% power for such changes. For the comparison of LCD vs OS groups, there is an 80% estimated power to detect a difference in effects on FPG of 0.6 mmol/l and on HOMA-IR of 2.6 units, respectively. A p value <0.05 was considered statistically significant, with no multiple testing correction. All data were analysed with IBM SPSS software version 23 (USA) and GraphPad Prism 10.0.2 (USA).
Results
In total, 24 participants completed the study: 15 were randomised to OS (one male, 14 female) and nine to LCD (one male, eight female) (Fig. 1). Of the 15 participants in the OS group, 11 underwent RYGB and 4 SG. Anthropometric and other clinical characteristics of the cohort at baseline and after intervention are shown in Table 1. The two groups were very similar in age, sex distribution, BMI, waist-to-height ratio and body fat %. In addition, they presented comparable glucose metabolism characteristics, including HbA1c, fasting glucose and M value at baseline. However, the LCD group had higher levels of fasting triglycerides and lower aspartate aminotransferase (AST) levels and hip circumference (Table 1). There were no serious or unexpected adverse effects following either of the interventions, and all participants completed the study. During post-surgery OGTT, nine participants experienced early dumping symptoms, e.g. nausea, blood pressure drop and diarrhoea, and this is an expected and well-known phenomenon after RYGB.
Clinical effects on anthropometric measures
Surgery and LCD led to comparable reductions in body weight and BMI (Table 1, Fig. 2). In both groups, the mean weight loss was 8–9 kg (7–8%) over the study period of 4 weeks. Accordingly, waist circumference was decreased by ~6 cm in both groups (Table 1). Moreover, body fat %, as assessed by bioimpedance analyses, was significantly decreased by OS and was decreased (albeit not significantly) by LCD (Table 1, Fig. 2c). There was a corresponding increase in LBM %, which was significant in the OS group (Table 1). Systolic BP was significantly reduced, and diastolic pressure was non-significantly reduced, by OS and LCD to a similar degree.

Anthropometric effects of OS (surgery) and LCD on BMI (a, d), body weight (b, e) and body fat % (c, f). Data are means ± SEM; individual values as indicated. Statistical methods and significances are given in Table 1. *p<0.05 and ***p<0.001
The level of physical activity assessed by 24 h accelerometer monitoring did not show any significant change after either OS or LCD and, thus, there were no differences between the groups. Further, the estimated 24 h energy expenditure (representing normal life, resting and active) did not show any differences between OS and LCD (Table 1). However, these analyses could be performed only in a subset of participants and therefore must be interpreted with caution.
Clinical effects on glucose and lipid levels and clinical biochemistry
Circulating glucose levels, reflected by HbA1c, were reduced more markedly by surgery than LCD at 4 weeks (Table 1), with the change from baseline differing significantly when comparing OS with LCD (p<0.01). Additionally, fasting glucose and insulin were reduced after OS (p<0.01) but not after LCD, with no significant differences in changes from baseline when comparing OS with LCD. The AUC for glucose, insulin and C-peptide concentrations were obtained during an OGTT (AUCOGTT; Fig. 3). Glucose AUCOGTT was increased by 20% after OS (p<0.001) but not after LCD, and this effect was independent of weight loss (%). Insulinogenic index was slightly reduced after surgery and significantly reduced in the LCD group (Fig. 4e,f), whereas insulin AUCOGTT was unaffected by either of the interventions (Table 1, Fig. 3d–f). The lipid levels, including fasting plasma cholesterol, HDL-cholesterol, LDL-cholesterol and triglycerides were reduced in both groups with no significant difference between the groups.

OGTT responses to OS (surgery) and LCD for glucose (a–c), insulin (d–f) and C-peptide (g–i). Data are mean ± SEM; individual values as indicated. Statistical method and significances are given in Table 1. **p<0.01 and ***p<0.001

Impact of OS (surgery) and LCD on indices of insulin sensitivity and secretion, in the fasting state (a, b) or during OGTT (c–h). Data are mean ± SEM of % change; individual values as indicated. *p<0.05, **p<0.01
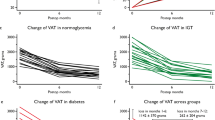
At baseline, seven individuals in the LCD group were diagnosed with prediabetes (either impaired fasting glucose or impaired glucose tolerance) and one of them reversed to a normoglycaemic condition following the diet (Fig. 5). Ten individuals in the OS group had prediabetes before surgery, and four of them reverted to normoglycaemia after the intervention. There was a nominally greater (but not significantly so), proportion of participants with prediabetes that converted to normoglycaemia (40%) in the OS group than in the LCD group (14%).

Number of participants with normoglycaemia (black) or prediabetes (impaired fasting glucose or impaired glucose tolerance, grey) before and after OS and LCD
C-reactive protein and AST were reduced by surgery but not by LCD (Table 1). The impact of OS on reduction of C-reactive protein was independent of weight loss. The interventions had different effects on creatinine (p=0.002), with OS reducing levels but LCD increasing levels (p<0.05).
Glucose homeostasis indices
Neither intervention significantly affected whole-body insulin sensitivity at 4 weeks, as assessed by the clamp-derived M value (Table 1). HOMA-IR was significantly reduced following OS (−26.3% [95% CI −49.5, −3.0], p=0.009); the reduction was not statistically significant following LCD (−20.9% [95% CI −58.2, 16.5]). Similar results were found for disposition index, indicating a possible insulin sensitisation effect. There were no consistent effects on the Matsuda index during a glucose load, and no significant difference between interventions regarding these indices could be detected (Table 1, Fig. 4).
Body and tissue composition assessed by MRI
Both OS and LCD caused significant decreases in magnetic resonance-derived estimates of whole-body, adipose tissue and non-adipose tissue volumes (all p<0.001, Table 2). Adipose tissue volume was comparably decreased by around 7% after both interventions. However, OS led to a greater decrease in non-adipose tissue volume (p<0.01), and this was independent of weight loss. Both surgery and LCD markedly decreased liver fat % by approximately 2% units. Neither intervention affected pancreas fat % (Table 2).
Whole-body and tissue-specific glucose turnover assessed by PET
There was a non-significant reduction in Rd during steady-state hyperinsulinaemic–euglycaemic clamp following LCD (p=0.09). EGP remained unaltered after both interventions (Table 2). Following OS, there was a decrease in tissue-specific glucose uptake rate in the heart (MRglu heart, p<0.001) and abdominal adipose tissue (p<0.05), whereas there was an increase in the skeletal muscles of the legs (p<0.05). Neither of these effects was seen after LCD, and neither of the interventions affected glucose uptake rates in any of the other assessed tissues (i.e. brain or liver) (Table 2, Fig. 6). However, LCD led to a non-significant increase in the glucose uptake rate of the brain (Table 2).

18F-FDG net influx rate Ki images depict whole-body glucose uptake rate (MRglu) during clamp steady state. Examples from the surgery group (a) and from the LCD group (b) are shown before (Pre) and after (Post) the respective intervention. The colour-bar indicates Ki values. Tissue-specific glucose uptake is quantified for brain, liver, heart, abdominal adipose tissue and leg muscles and are shown in Table 2
Correlation and sensitivity analyses
Reduction of fasting plasma glucose after intervention was positively associated with absolute and relative body weight loss following OS but not LCD (ESM Table 1). Furthermore, lowering of EGP was associated with body fat reduction, although this was significant only in the LCD group. The body fat % reduction negatively correlated with the liver fat reduction in the OS group, while in the LCD group, this association was positive (both p<0.05). No correlations were found between weight loss and glycaemic or 18F-FDG-PET/MRI-derived effect measures.
The two types of OS, RYGB and SG, lead to weight loss by partly differing mechanisms and they also display different effects on long-term diabetes remission and weight maintenance. Therefore, we performed separate sensitivity analyses by including only the larger subgroup undergoing RYGB. The short-term effects on glycaemia, insulin sensitivity, whole-body and tissue-specific fat content, and glucose turnover remained very similar, as did the limited differences when compared with LCD (data not shown).
Discussion
This is the first study that directly compares the short-term effects of OS and LCD on tissue-specific glucose turnover and body composition. The early effects are of specific interest since OS rapidly improves glucose homeostasis (within a few days) in individuals with or without prior diabetes [11, 32], while LCDs can achieve similar effects but over several months [33]. We addressed body composition, glucose control and insulin action at both whole-body and tissue level in individuals with obesity and no diabetes. Integrated PET/MRI investigations during hyperinsulinaemic–euglycaemic clamps were conducted before and after the interventions. The two interventions exhibited partly similar short-term metabolic effects. However, despite nearly identical weight loss, there were some interesting differences: increased glucose uptake in skeletal muscle but reduced uptake in the heart and abdominal adipose tissue occurred after OS but not after an LCD.
Clinical effects
OS and LCD induced a similar reduction in body weight (8–9 kg) 4 weeks after the intervention. Both groups of participants experienced comparable reductions in circulating lipids and BP, whereas fasting plasma glucose, insulin, HbA1c and HOMA-IR were reduced more markedly, or only, following OS. After OS, a higher proportion of participants with prediabetes (impaired glucose tolerance or impaired fasting glucose) reverted to normoglycaemia, with four out of 10 (40%) becoming normoglycaemic compared with one out of seven (14%) for LCD. Taken together, the data support the notion that dysglycaemia normalises more rapidly after OS than after an LCD, and that this difference is independent of weight loss [11, 32].
Body composition
OS and LCDs similarly reduced whole-body adipose tissue volume by about 7%, along with a reduction in liver fat content by 2% units, whereas pancreas fat did not change in either group. Interestingly, the participants that underwent OS exhibited a slightly greater volume reduction in non-adipose tissues than those given the LCD, suggesting a relatively greater loss of fluid from non-adipose vs adipose tissue in the OS compared with the LCD group. This has previously been reported as a rapid and possibly temporary effect following OS, although the mechanisms are not clear [34, 35].
Liver fat content was reduced similarly following both interventions; in the LCD group, this was positively correlated with the reduction in whole-body fat %. In contrast, the opposite was found with OS (i.e. a significant inverse relationship between whole-body and liver fat reduction). This might be explained by enhanced lipid release from adipose tissue, potentially leading to elevated uptake in the liver [36], which could in turn drive hepatic insulin resistance. Nonetheless, there was a net decrease in liver fat following OS, in keeping with lower HOMA-IR and fasting plasma glucose. Furthermore, the rapid decrease in fasting glucose and hepatic insulin resistance following OS is probably also due to several other factors, including resetting of secretion of incretins and other glucose-regulating hormones as well as adaptative changes of the brain’s glucose-sensing and regulating functions [16, 17, 29].
Glucose turnover
In the OS group, there was a 20% increase in glucose AUC in response to an OGTT, in contrast to the LCD group. This result is likely attributed to the anatomical rearrangements specifically in RYGB patients, in whom the duodenum and much of the stomach are bypassed, allowing for rapid glucose absorption in the jejunum. During hyperinsulinaemia, only the OS group showed a significantly increased PET-derived glucose uptake in skeletal muscle (by about 25%). OS also led to a substantial 40% reduction in glucose uptake in the heart and a 10% reduction in abdominal adipose tissue, with no significant changes in the brain or liver.
Surprisingly, Rd and EGP were unaffected by either intervention. Previous work has shown reduced EGP post-RYGB, often under fasting conditions or at later time points than four weeks [37, 38]. Our data suggest a probable reduction in fasting EGP following RYGB, as evidenced by decreased fasting glucose and HOMA-IR. This implies that the glucose-lowering effect of OS is more related to fasting conditions than the fed state. At 4 weeks after OS, no clear improvements in glucose metabolism, insulin secretion or insulin action upon an oral glucose load were observed, as Matsuda and insulinogenic indices remained unchanged. This aligns with unaltered PET-derived glucose uptake at the whole-body level during hyperinsulinaemia. Nevertheless, the increased glucose uptake rate in skeletal muscle and adipose tissue supports the occurrence of rapid tissue-specific insulin sensitisation after OS [39].
Integrated assessment
The outcomes of insulin sensitivity assessments displayed variability across diverse methods. Notably, the clamp experiments, coupled with PET/MRI investigations, reflected a submaximal insulin-stimulated state, a characteristic largely shared with the Matsuda index derived from OGTT data. Examining the impact of OS on insulin-stimulated glucose uptake in tissues, using FDG-PET, revealed distinctive patterns: an increased uptake in skeletal muscle and adipose tissue, and a reduced uptake in the heart. However, there were no significant changes in the whole-body glucose turnover, and those effects were also found following an LCD. In contrast, HOMA-IR reflects the fasting condition and suggests a more marked improvement of insulin resistance after OS.
Increased insulin sensitivity of skeletal muscle probably explains the observed increase in its glucose utilisation at 4 weeks after OS, as previously observed in other studies [40]. However, our data also revealed that glucose uptake was reduced in adipose tissue and myocardium. The latter might be due to lower cardiac output [41] and hence less strain on the heart. We hypothesise that the rapid glycaemic improvement after OS is mainly accounted for by reduced hepatic glucose production in the fasting state. However, this hypothesis was not directly addressed as EGP was only measured during hyperinsulinaemic clamps and did not change. Albeit direct measurements were not performed, the notion of lowered EGP during fasting [38], and thus much of everyday life, is supported by the observed reduction in HOMA-IR after OS. Notably, at later time points after OS, there are clear effects also on whole-body glucose utilisation during hyperinsulinaemia [17, 42].
Our correlation analyses indicate that the magnitude of body weight loss does not directly impact the rapid changes in glycaemic regulation. This is also supported by the lowering of glycaemic measures seen 4 weeks after OS but not LCD, despite similar body weight and fat loss. Thus, we propose that, after OS compared with LCD, there is a more rapid change of fasting plasma glucose and this may be mediated by a lower hepatic glucose production in the fasting state, which could not be assessed during our hyperinsulinaemic clamps.
We observed no evident effects on whole-body insulin action during the clamps, as reflected by the M value (glucose infusion rate) and glucose uptake rates derived from FDG-PET. This finding was unexpected as both weight loss per se and, in particular, OS are known to markedly reverse insulin resistance. However, it seems likely that those effects require several months to manifest. This was previously shown by us and others and may involve adipose tissue remodelling and accompanying functional changes including insulin responsiveness and altered gene expression [12, 17]. Moreover, the brain and neuroendocrine pathways may play an important role. Attenuated insulin-antagonistic neurohormonal responses (adrenocorticotropic hormone, cortisol, glucagon, growth hormone and sympathoadrenergic) have been shown by us and others following RYGB [16, 43]. Within the brain, glucose utilisation, as well as blood flow and neural network activity, is changed and these alterations likely contribute to the resetting of whole-body glucose metabolism. Such effects (e.g. a general reduction in brain glucose uptake) were demonstrated after at least 4 months and thus may not operate earlier [16, 29, 44]. This is supported by our present finding of an unchanged rate of glucose uptake in the whole brain after both OS and LCD. However, this does not preclude some changes in critical brain regions or effects on other brain functions.
Strengths and limitations
This study is the first to compare the short-term metabolic effects of OS and LCD with a comprehensive assessment of tissue-specific and whole-body glucose turnover. Integrated simultaneous PET/MRI imaging was employed for the measurement of body composition, fat distribution and quantitative assessment of glucose fluxes. Notably, PET/MRI offers advantages over the more commonly available and less costly PET/computed tomography (CT) method, thanks to its lower radiation dose for whole-body investigations. Furthermore, MRI enables more precise quantifications such as liver fat compared with CT [45]. While our study provides valuable insights, we acknowledge inherent limitations due to the modest sample size, which was due to challenges in participant recruitment and resource constraints, in turn posed by the complex and cumbersome investigations. Consequently, there is low statistical power to detect minor differences in effects between the two interventions. Additionally, since most of the participants in the study were female, generalisations to all sex and genders in the populations is limited.
Of note, we only address the first 4 weeks after interventions. Repeated follow-up investigations would be of interest but were hindered by the waiting list design (with surgery performed directly after the study in the LCD group) and also by radiation exposure limits. At this point, we have not analysed incretin hormones, which may be involved in the early effects on glucose homeostasis, particularly following OS where enhanced responses to oral glucose are found [12, 44]. However, stimulated insulin secretion during OGTT was not amplified following either treatment, so the role of incretins in short-term glycaemic changes may be limited. In future work, we will address gut hormone regulation after LCD and RYGB. Quantitative glucose partitioning to different tissues should also be explored in more detail but would require rather challenging volume determination of each tissue of interest [26].
Conclusions
While achieving identical weight loss, OS and LCD also led to similar reductions in whole-body and liver fat after 4 weeks. However, only surgery increased the glucose uptake rate in skeletal muscle during hyperinsulinaemia, whereas it reduced the uptake rate in the myocardium and abdominal adipose tissue. Both liver and brain glucose uptake rates were similar between OS and LCD, as were whole-body glucose uptake and EGP. Taken together, the data indicate that the short-term metabolic effects of OS are not explained by loss of body fat alone. Although the full effects on whole-body insulin resistance and blood glucose levels do not occur immediately, there are clear reductions in fasting plasma glucose and insulin resistance as well as in HbA1c as early as 4 weeks post-OS, potentially contributing to the prevention or reversal of type 2 diabetes. This indicates a specific and rapid glucose-lowering effect of OS, probably mainly explained by lower glucose production by the liver in the non-fed condition.
Abbreviations
- AST:
-
Aspartate aminotransferase
- CONSORT:
-
Consolidated Standards of Reporting Trials
- CT:
-
Computed tomography
- EGP:
-
Endogenous glucose production
- 18F-FDG:
-
[18F]fluorodeoxyglucose
- IDEAL-IQ:
-
Iterative decomposition of fat and water with echo asymmetry and least squares estimation
- LBM:
-
Lean body mass
- LCD:
-
Low-energy (low-calorie) diet
- MRAC:
-
Magnetic resonance attenuation correction
- MRglu:
-
Tissue glucose metabolic rate
- OS:
-
Obesity surgery
- PET:
-
Positron emission tomography
- Rd:
-
Glucose disposal
- RYGB:
-
Roux-en-Y gastric bypass
- SAT:
-
Subcutaneous adipose tissue
- SG:
-
Sleeve gastrectomy
References
Pereira MJ, Eriksson JW, Svensson MK (2014) A case report of improved metabolic control after conversion from everolimus to cyclosporin A: role of adipose tissue mechanisms? Transplant Proc 46(7):2377–2380. https://doi.org/10.1016/j.transproceed.2014.02.018
Chooi YC, Ding C, Magkos F (2019) The epidemiology of obesity. Metabolism 92:6–10. https://doi.org/10.1016/j.metabol.2018.09.005
Després JP, Lemieux I (2006) Abdominal obesity and metabolic syndrome. Nature 444(7121):881–887. https://doi.org/10.1038/nature05488
Höskuldsdottir G, Engström M, Rawshani A et al (2022) Comparing effects of obesity treatment with very low energy diet and bariatric surgery after 2 years: a prospective cohort study. BMJ Open 12(4):e053242. https://doi.org/10.1136/bmjopen-2021-053242
Muller TD, Bluher M, Tschop MH, DiMarchi RD (2022) Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov 21(3):201–223. https://doi.org/10.1038/s41573-021-00337-8
Ma C, Avenell A, Bolland M et al (2017) Effects of weight loss interventions for adults who are obese on mortality, cardiovascular disease, and cancer: systematic review and meta-analysis. BMJ 359:j4849. https://doi.org/10.1136/bmj.j4849
Sjostrom L, Narbro K, Sjostrom CD et al (2007) Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 357(8):741–752. https://doi.org/10.1056/NEJMoa066254
Nguyen NT, Varela JE (2017) Bariatric surgery for obesity and metabolic disorders: state of the art. Nat Rev Gastroenterol Hepatol 14(3):160–169. https://doi.org/10.1038/nrgastro.2016.170
Halliday TM, Polsky S, Schoen JA et al (2019) Comparison of surgical versus diet-induced weight loss on appetite regulation and metabolic health outcomes. Physiol Rep 7(7):e14048. https://doi.org/10.14814/phy2.14048
Svanevik M, Lorentzen J, Borgeraas H et al (2023) Patient-reported outcomes, weight loss, and remission of type 2 diabetes 3 years after gastric bypass and sleeve gastrectomy (Oseberg); a single-centre, randomised controlled trial. Lancet Diabetes Endocrinol 11(8):555–566. https://doi.org/10.1016/S2213-8587(23)00127-4
Bradley D, Magkos F, Klein S (2012) Effects of bariatric surgery on glucose homeostasis and type 2 diabetes. Gastroenterology 143(4):897–912. https://doi.org/10.1053/j.gastro.2012.07.114
Katsogiannos P, Kamble PG, Boersma GJ et al (2019) Early changes in adipose tissue morphology, gene expression, and metabolism after RYGB in patients with obesity and T2D. J Clin Endocrinol Metab 104(7):2601–2613. https://doi.org/10.1210/jc.2018-02165
Cadena-Obando D, Ramírez-Rentería C, Ferreira-Hermosillo A et al (2020) Are there really any predictive factors for a successful weight loss after bariatric surgery? BMC Endocr Disord 20(1):20. https://doi.org/10.1186/s12902-020-0499-4
Karra E, Yousseif A, Batterham RL (2010) Mechanisms facilitating weight loss and resolution of type 2 diabetes following bariatric surgery. Trends Endocrinol Metab 21(6):337–344. https://doi.org/10.1016/j.tem.2010.01.006
Cordera R, Adami GF (2016) From bariatric to metabolic surgery: looking for a “disease modifier” surgery for type 2 diabetes. World J Diabetes 7(2):27–33. https://doi.org/10.4239/wjd.v7.i2.27
Almby KE, Lundqvist MH, Abrahamsson N et al (2021) Effects of gastric bypass surgery on the brain: simultaneous assessment of glucose uptake, blood flow, neural activity, and cognitive function during normo- and hypoglycemia. Diabetes 70(6):1265–1277. https://doi.org/10.2337/db20-1172
Almby KE, Katsogiannos P, Pereira MJ et al (2021) Time course of metabolic, neuroendocrine, and adipose effects during 2 years of follow-up after gastric bypass in patients with type 2 diabetes. J Clin Endocrinol Metab 106(10):e4049–e4061. https://doi.org/10.1210/clinem/dgab398
Castro-Barquero S, Ruiz-Leon AM, Sierra-Perez M, Estruch R, Casas R (2020) Dietary strategies for metabolic syndrome: a comprehensive review. Nutrients 12(10):2983. https://doi.org/10.3390/nu12102983
Jensen MD, Ryan DH, Apovian CM et al (2014) 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults. Circulation 129(25_suppl_2):S102–S138. https://doi.org/10.1161/01.cir.0000437739.71477.ee
Franz MJ, VanWormer JJ, Crain AL et al (2007) Weight-loss outcomes: a systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J Am Diet Assoc 107(10):1755–1767. https://doi.org/10.1016/j.jada.2007.07.017
Dombrowski SU, Knittle K, Avenell A, Araújo-Soares V, Sniehotta FF (2014) Long term maintenance of weight loss with non-surgical interventions in obese adults: systematic review and meta-analyses of randomised controlled trials. BMJ 348:g2646. https://doi.org/10.1136/bmj.g2646
Salem V, Demetriou L, Behary P et al (2021) Weight loss by low-calorie diet versus gastric bypass surgery in people with diabetes results in divergent brain activation patterns: a functional MRI study. Diabetes Care 44(8):1842–1851. https://doi.org/10.2337/dc20-2641
Zubrzycki A, Cierpka-Kmiec K, Kmiec Z, Wronska A (2018) The role of low-calorie diets and intermittent fasting in the treatment of obesity and type-2 diabetes. J Physiol Pharmacol 69(5):663–683. https://doi.org/10.26402/jpp.2018.5.02
Schulz KF, Altman DG, Moher D (2010) CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. J Pharmacol Pharmacother 1(2):100–107. https://doi.org/10.4103/0976-500X.72352
Campos GM, Rabl C, Peeva S et al (2010) Improvement in peripheral glucose uptake after gastric bypass surgery is observed only after substantial weight loss has occurred and correlates with the magnitude of weight lost. J Gastrointest Surg 14(1):15–23. https://doi.org/10.1007/s11605-009-1060-y
Eriksson JW, Visvanathar R, Kullberg J et al (2021) Tissue-specific glucose partitioning and fat content in prediabetes and type 2 diabetes: whole-body PET/MRI during hyperinsulinemia. Eur J Endocrinol 184(6):879–889. https://doi.org/10.1530/EJE-20-1359
Boersma GJ, Johansson E, Pereira MJ et al (2018) Altered glucose uptake in muscle, visceral adipose tissue, and brain predict whole-body insulin resistance and may contribute to the development of type 2 diabetes: a combined PET/MR study. Horm Metab Res 50(8):e10. https://doi.org/10.1055/a-0831-3620
Johansson E, Lubberink M, Heurling K et al (2018) Whole-body imaging of tissue-specific insulin sensitivity and body composition by using an integrated PET/MR system: a feasibility study. Radiology 286(1):271–278. https://doi.org/10.1148/radiol.2017162949
Rebelos E, Immonen H, Bucci M et al (2019) Brain glucose uptake is associated with endogenous glucose production in obese patients before and after bariatric surgery and predicts metabolic outcome at follow-up. Diabetes Obes Metab 21(2):218–226. https://doi.org/10.1111/dom.13501
Lundkvist P, Pereira MJ, Katsogiannos P, Sjostrom CD, Johnsson E, Eriksson JW (2017) Dapagliflozin once daily plus exenatide once weekly in obese adults without diabetes: sustained reductions in body weight, glycaemia and blood pressure over 1 year. Diabetes Obes Metab 19(9):1276–1288. https://doi.org/10.1111/dom.12954
Lundqvist MH, Pereira MJ, Almby K, Hetty S, Eriksson JW (2024) Regulation of the cortisol axis, glucagon, and growth hormone by glucose is altered in prediabetes and type 2 diabetes. J Clin Endocrinol Metab 109(2):e675–e688. https://doi.org/10.1210/clinem/dgad549
Gudbrandsen OA, Dankel SN, Skumsnes L et al (2019) Short-term effects of vertical sleeve gastrectomy and Roux-en-Y gastric bypass on glucose homeostasis. Sci Rep 9(1):14817. https://doi.org/10.1038/s41598-019-51347-x
Lean ME, Leslie WS, Barnes AC et al (2018) Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 391(10120):541–551. https://doi.org/10.1016/S0140-6736(17)33102-1
Haghighat N, Ashtary-Larky D, Bagheri R et al (2022) Preservation of fat-free mass in the first year after bariatric surgery: a systematic review and meta-analysis of 122 studies and 10,758 participants. Surg Obes Relat Dis 18(7):964–982. https://doi.org/10.1016/j.soard.2022.02.022
Nuijten MAH, Monpellier VM, Eijsvogels TMH, Janssen IMC, Hazebroek EJ, Hopman MTE (2020) Rate and determinants of excessive fat-free mass loss after bariatric surgery. Obes Surg 30(8):3119–3126. https://doi.org/10.1007/s11695-020-04654-6
Immonen H, Hannukainen JC, Kudomi N et al (2017) Increased liver fatty acid uptake is partly reversed and liver fat content normalized after bariatric surgery. Diabetes Care 41(2):368–371. https://doi.org/10.2337/dc17-0738
Camastra S, Gastaldelli A, Mari A et al (2011) Early and longer term effects of gastric bypass surgery on tissue-specific insulin sensitivity and beta cell function in morbidly obese patients with and without type 2 diabetes. Diabetologia 54(8):2093–2102. https://doi.org/10.1007/s00125-011-2193-6
Flynn CR, Albaugh VL, Tamboli RA et al (2020) Roux-en-Y gastric bypass surgery improves hepatic glucose metabolism and reduces plasma kisspeptin levels in morbidly obese patients with type 2 diabetes. Am J Physiol Gastrointest Liver Physiol 318(2):G370–G374. https://doi.org/10.1152/ajpgi.00224.2019
Dadson P, Landini L, Helmio M et al (2016) Effect of bariatric surgery on adipose tissue glucose metabolism in different depots in patients with or without type 2 diabetes. Diabetes Care 39(2):292–299. https://doi.org/10.2337/dc15-1447
Morbelli S, Marini C, Adami GF et al (2013) Tissue specificity in fasting glucose utilization in slightly obese diabetic patients submitted to bariatric surgery. Obesity (Silver Spring) 21(3):E175-181. https://doi.org/10.1002/oby.20003
Almby KE, Abrahamsson N, Lundqvist MH et al (2019) Effects of GLP-1 on counter-regulatory responses during hypoglycemia after GBP surgery. Eur J Endocrinol 181(2):161–171. https://doi.org/10.1530/EJE-19-0171
Pournaras DJ, Nygren J, Hagström-Toft E, Arner P, le Roux CW, Thorell A (2016) Improved glucose metabolism after gastric bypass: evolution of the paradigm. Surg Obes Relat Dis 12(8):1457–1465. https://doi.org/10.1016/j.soard.2016.03.020
de Heide LJM, van den Broek M, van Dijk G, Emous M, van Beek AP (2021) Diminished counterregulatory responses to meal-induced hypoglycemia 4 years after RYGB. Obes Surg 31(2):597–602. https://doi.org/10.1007/s11695-020-05035-9
Fanni G, Katsogiannos P, Nandi Jui B et al (2022) Response of multiple hormones to glucose and arginine challenge in T2DM after gastric bypass. Endocr Connect 11(8):e220172. https://doi.org/10.1530/EC-22-0172
Zhang YN, Fowler KJ, Hamilton G et al (2018) Liver fat imaging-a clinical overview of ultrasound, CT, and MR imaging. Br J Radiol 91(1089):20170959. https://doi.org/10.1259/bjr.20170959
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Acknowledgements
We thank all staff involved in the study from all collaborating departments of Uppsala University and Uppsala University Hospital. We are also grateful to the patients for participating in the uncomfortable and time-consuming investigations.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding authors upon reasonable request.
Funding
Open access funding provided by Uppsala University. This work was supported by research grants from AstraZeneca R&D, the Swedish Diabetes Foundation, the European Union’s Horizon Europe Research project PAS GRAS under grant agreement no. 101080329, the European Commission via the Marie Sklodowska Curie Innovative Training Network TREATMENT (H2020-MSCA-ITN-721236), EXODIAB, the Family Ernfors Foundation, the P.O. Zetterling Foundation, Novo Nordisk Foundation (NNF20OC0063864, NNF23OC0084483), the Agnes and Mac Rudberg Foundation and the Uppsala University Hospital ALF grants.
Authors’ relationships and activities
BCLC is an employee at Astra Zeneca R&D. The other authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work.
Contribution statement
JWE, HA and UR conceived and designed the research. The investigation phase involved MJP, CK, SK, EL, BCLC, MS, ST, MHL, JK, ML and UR. JWE, MJP, CK, GF and SK contributed to formal analyses and interpretation of the data. JWE, HA and MJP received funding. JWE, MJP, CK, SK, EL, GF, ML, ST, JK and UR drafted the paper. All authors critically revised and approved the final version to be submitted. JWE and HA are the guarantors of this work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eriksson, J.W., Pereira, M.J., Kagios, C. et al. Short-term effects of obesity surgery versus low-energy diet on body composition and tissue-specific glucose uptake: a randomised clinical study using whole-body integrated 18F-FDG-PET/MRI. Diabetologia (2024). https://doi.org/10.1007/s00125-024-06150-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00125-024-06150-3